
{kind=link}
Editor’s note: Note clarification (marked in the text) in the Appendix.
Abigail Shrier’s 2020 book, Irreversible Damage, is a call to arms for parents of “teens who are lured into “trans ideology”. Shrier bases her arguments in parental anecdotes and bolsters her claims with cherry-picked research, interviewing only those professionals who support her narrative. For context, see Part One of this review.
Here, we will discuss “gender ideology” objectives as interpreted by Shrier; mental health approaches to gender dysphoria; social, medical, and surgical aspects of gender affirmation; Shrier’s solutions to the transgender “craze”; and review the bedrock of beliefs Shrier’s book is built on, as built by her sources and the “experts” whom she interviews.
“Gender ideology” part 1: Turn all the lesbians into trans men
Masculine and/or gay women are disappearing, Shrier warns; modern lesbian teens are “becoming” trans instead.
As Shrier describes it, “many of the girls now being cornered into a trans identity might, in an earlier era, have come out as gay”. This argument is not new, in fact, it is firmly rooted in the gender critical (or trans-exclusionary) community. Gender critical people are those who don’t believe that trans women are women, fight for exclusion of trans women from women’s spaces, and are vocal against trans rights legislation. They may be inclusive of trans men, but only because they gender them as women. Shrier writes, “gender ideology puts transgender individuals into direct conflict with radical feminists who believe sex is the defining feature of one’s identity”.
Actor Elliot Page came out as trans on Dec. 1, 2020:
— Elliot Page (@TheElliotPage) December 1, 2020
In response, he received transphobic messages from both lesbians and gender critical feminists (and lesbian gender critical feminists) mourning the “loss” to and “betrayal” of their community. Those who expressed these sentiments misgendered and deadnamed Elliot in their posts, claiming that young lesbians are encouraged to identify as heterosexual trans men:
Elliot is a queer, non-binary trans guy; the claim is baseless.
One of the desisters that Shrier interviews wonders why her gender therapist wouldn’t just say, “no, you’re not trans, you’re a lesbian“. Shrier builds on this: “many detransitioning young women have since come to believe they were just young lesbians who had internalized homophobia and been led to believe that not being typically feminine meant they weren’t female at all. Nearly all of them struggled with mental health and engaged in self-harm.”
There is no evidence to support the claim that today’s AFAB youth are more frequently identifying as trans and less frequently identifying as lesbian. The 2020 Gallup survey finds that the vast majority Gen-Z teenagers identify as heterosexual (78.9%) but among the 21.1% within the LGBTQ group, the majority identify as bisexual (11.5%). Approximately 1.4% identify as lesbian and 2.1% as gay. Transgender respondents, reported at 1.8%, were not separated by their assigned sex at birth, meaning that the 1.8% ratio consists of both AFAB and AMAB people, a fact overlooked by those who use the data to claim lesbian erasure in favor of trans identity:
Finally, as famed lesbian @kittypurrzog notes, there are now — among Millennials and Gen Z — more people identifying as trans than lesbian. She has previously argued that masculine girls are now encouraged to identify as trans, causing a decrease in the lesbian population: pic.twitter.com/stFNHQtLoq
— Glenn Greenwald (@ggreenwald) February 24, 2021
Two facts topple this assertion: First, the same study notes that, compared to millennials, the proportion of Gen Z that identifies as trans has grown by 50%, and the proportion that identifies as lesbian has grown by 75%. Second, trans identity is not a sexual orientation, and trans respondents may also have (and likely did) identify themselves as gay, lesbian, and bisexual. In fact, the majority of trans youth identify as queer.
The internalized homophobia argument, a well-worn trope, does not track when reviewing the statistics. Why would lesbians become heterosexual trans men when most AFAB transmasculine youth are not straight?
To briefly address Shrier’s assertions: gender expression is not gender identity; transmasculine people can be feminine (whatever that means). Mental health concerns endorsed by trans adults are largely recognized to be attributed to minority stress. Up to this date, research has focused on mental health interventions for trans youth, but smaller studies have indicated a similar pattern for youth as for adults as far as minority stress is concerned. The Gender Minority Stress and Resilience Measure was recently updated with an adolescent extension inclusive of trans youth.
Population surveys from 2008 to 2019 have consistently identified a lesbian population of 0.9% to 4%. Gen Z’s 1.4% lesbian identification is the highest it has ever been in any generation.
Shrier advises: “don’t be afraid to admit: it’s wonderful to be a girl.” Well, sure, if you are one.
Being lesbian, Shrier informs us, has “less cachet” than being trans for today’s teens. Is it “cachet” to be targeted in school sports? Villainized in the news and mischaracterized by the media? Is it “cachet” to be denied medical care?
{kind=link}
“Gender ideology” part 2: Tell kids to become trans, they’ll be insta-popular
According to Shrier, the internet is saturated with gender ideology luring in misguided, lonely youth with promises of love and praise. She describes a subject who cut off their parents in favor of friends and social media. The parents told their child that their identity didn’t “match” their history, that biology is what makes them a woman, and characterized gender identity affirmation as an “apparent fixation”. The parents found their child’s post-top surgery Instagram post, in which the youth expressed joy and happiness. The post was met with love and support from friends and followers. “You know–the usual” the parents report as Shrier consoles them. To these parents and to Shrier, gender affirmation is a mistake, regardless of their child’s sense of happiness. Shrier bolsters her assertion with Littman’s ROGD study, in which parents were asked about and confirmed an increase in their children’s social media use prior to their children coming out as trans.
YouTube, Instagram, Tumblr, Reddit, Twitter, Facebook, DeviantArt, and Tiktok are all “popular hubs” for giving tips on being trans and getting hormones, and for “seething over transphobia”, Shrier warns. She weaponizes social media against trans youth by asserting that queer representation in media makes teens trans. She mischaracterizes spaces that youth may turn to for support as spaces of indoctrination in gender ideology (which Shrier also recently compared to critical race theory.) Media can be an escape from a heteronormative world, empowering teens with positive representation and visibility in light of discrimination and isolation. Social media can provide a sense of belonging in a world where sexual and gender minorities are derided and harassed by their families and schools. Online spaces are safe and anonymous and provide access to support and resources that may not be available otherwise. For those who can’t be themselves in real life, online spaces can be ones of self-expression and comfort.
In one study, a trans man identifies YouTube and Facebook as giving him hope. He writes that his mother thinks social media was a trigger: if it wasn’t there, he probably wouldn’t be trans. He counters, if it wasn’t there, I might have died by suicide.
Despite the benefits of social media, LGBTQ youth have a higher risk of being victims of online aggression and cyberbullying. Being trans in a social media space does not equal popularity.
LGBTQ youth report both positive (96%) and negative (88%) impacts from social media on their mental health and well-being.
Shrier notes the “increased popularity of Pride events”. Pride celebrations are about acceptance and equality in a world where LGBTQ people still fight for basic rights; they are about connection, community, and visibility. LGBTQ events are important to promote social justice and counter marginalization.
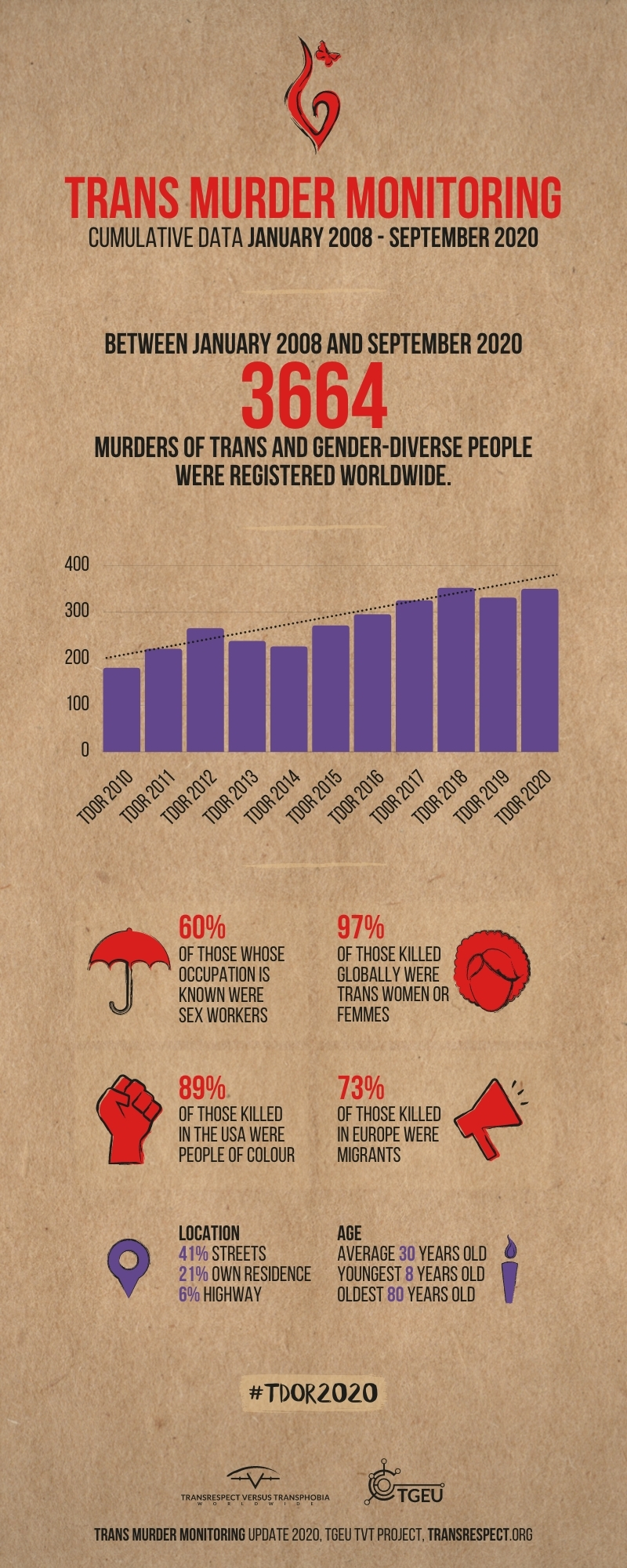
In 2020, 44 trans people were violently killed in the US, the highest figure since the Human Rights Campaign began tracking these statistics in 2013. According to data collected by the research branch of advocacy network Transgender Europe, at least 350 trans people worldwide were murdered between October 2019 and September 2020, representing a 6% increase in reported murders from 2019.
{kind=link}
Still, Shrier asserts that AFAB teens who come out as transgender garner instant popularity and support. With one subject, Shrier concludes that they “register(ed) the new chance at social acceptance”. She warns that an AFAB teen sharing their gender identity and sexual orientation online sends up ‘a flare to actual adults who will immediately contact her and offer “support,” primed to take advantage’.
This characterization of trans adults as predators is intentional.
Trans identity is fashionable, according to Shrier, and causes a “liberating tug of cross-sex identification.” The “acute isolation” of today’s AFAB teenagers means they “might want to take cover under an LGBTQ umbrella.”
Shrier does note, “as a group, transgender-identified students are no doubt a uniquely vulnerable population, saddled with higher rates of depression and suicide and likely more abused than non-trans-identified students.” Today’s cisgender girls may feel acute isolation, but studies on gender minority youth have consistently identified isolation as a major concern. What LGBTQ umbrella? The COVID-19 pandemic only deepened these disparities.
Which one is it? Are trans youth popular and cool, or are they vulnerable and abused?
“Gender ideology” part 3: Teach it in schools
To Shrier, women are being erased everywhere, even in history class: schools are now teaching students that those famous women in history who took on “traditionally male roles” (Shrier’s characterization) may have identified as gender non-conforming in our modern lexicon. Shrier writes, “None of these women thought she was less of a woman for having taken on traditionally male roles,” a speculative claim at best.
An LGBTQ-inclusive school curriculum is the exception, not the rule. Only six states require schools to teach an LGBTQ-inclusive history and social science curriculum. Currently there are five states in the US that prohibit positive portrayals of sexual (and, though not specified, often by extension, gender) minorities. This legislation, also known as the “no promo homo” law, dictates that education programs must state that homosexual conduct is a criminal offense and not an acceptable lifestyle. Another version, the “don’t say gay” law, disallows any mention of LGBTQ people in the curriculum. These laws have been enacted in a number of states since the late 1970s, with a surge during the HIV/AIDS epidemic. These laws are harmful to LGBTQ teachers and students.
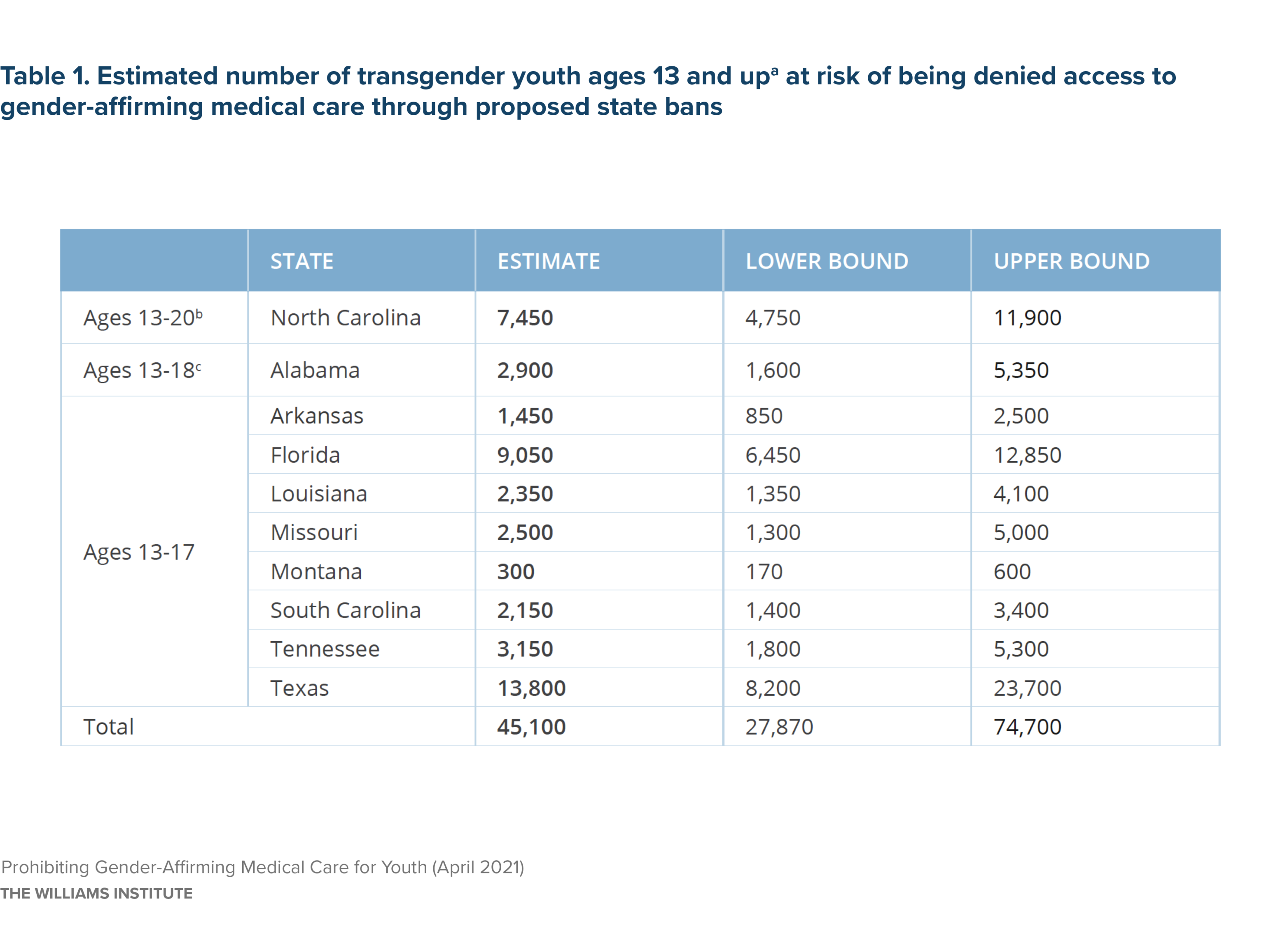
As of May 25, 2021, there were only 14 states with non-discrimination laws specific to LGBTQ students; the vast majority of states have no laws or policies to protect LGBTQ students. Over 250 anti-LGBTQ bills were introduced in state legislatures this year with others poised to be filed; a number of them specifically target trans students. Protections for trans students have been rolled back, and funding for schools to support trans youth withheld. In 2021, a year marked by the highest number of anti-trans bills in history, transphobia still guides major decisions around human rights.
Data from several studies of over 100,000 trans youth in the US shows that trans youth experience severe discrimination at school: 40% were physically harmed or threatened because of their gender identity. 20% attempted suicide in the previous year. They were 1.66 times more likely to get bullied at school. 77% of trans people surveyed were discriminated against at school. Nearly 1 in 4 trans kids change schools because they were harassed for being trans. 61% of trans youth reported being prevented or discouraged from using the bathroom corresponding to their gender identity. Trans students experience more hostility at school compared to cis LGB students.
“Gender ideology” part 4: Coach teens to say they’re suicidal so they can get hormones
Shrier notes that rates of suicidal ideation among trans people “are indeed startlingly high,” only to immediately cast aspersions on the statistics reported by several research studies. She speculates that the “rate is likely inflated because it is based on self-report,” a statement not endorsed by any of the studies. It is more likely that suicidal ideation and attempts are underreported; students may not disclose their gender identity for fear of discrimination and bullying, and there is a lack of systematic gender identity data collection. A recent meta-analytic review of worldwide (death by) suicide rates in youth only included binary male/female categories of gender identity. Only recently have large-scale, national studies begun to consider including trans demographics on death by suicide. A limitation there is that autopsy datasets can only collect what is known about an individual’s gender identity postmortem. A secondary analysis of National Violent Death Reporting System (NVDRS) found that 24% of 12-14 year olds who died by suicide were LGBT; these young ages had the greatest suicide disparity between LGBT and non-LGBT youth.
Trans teen suicide is met with dismissiveness; Shrier writes, ‘asking your (daughter) ‘are you out of your mind?’ is clearly off-limits, then…put out of your mind every manner of very understandable parental interjection. You don’t want your child to hang “himself” in the garage just because you accidentally referred to (her) as “Rebecca.”‘ (Quotation marks around himself are Shrier’s.)
To Shrier, the suicide (attempt) rate of 41% is part of the Trans Agenda’s “suicide narrative.” Trans suicide statistics are cruel parental manipulation, per Shrier: “there is one way any adolescent can bring parents to surrender: with a compelling threat of self-harm.” Lisa Marchiano, LCSW, agrees: “suicide statistics are employed in a manner that is both irresponsible and unethical.” Bailey and Blanchard agree and note that suicide and threats to commit suicide can be socially contagious.
4thWaveNow, a blog for and by people who question the “medicalization” of trans youth, is sourced frequently by Shrier. One of the parents interviewed for Shrier’s book is the site’s founder, and mother to an AFAB teen who detransitioned. The blog claims that the trans teen suicide attempt rate is closer to 20%. This is entirely speculative, and still high.
Studies note suicidal ideation rates in trans people between 39% and 48.5% in one year, with suicide attempts in trans youth at 29% within one year. Many potential variables lead to an increased suicide rate for trans youth; inflation of statistics by faking suicidal ideation is not one of them.
We can’t trust these teens, Shrier seems to conclude: they lie to get on hormones, lie about being trans, and blame their parents for not being supportive of the lies.
“Gender ideology” part 5: Separate teens from their parents
Shrier’s book is centered around the narratives of parents of AFAB trans youth. Her subjects, aside from those she identifies as detransitioners, were not involved in telling their own stories. Shrier sees herself the way she sees the experts interviewed for her book: a “lone sympathizer with parents facing the predicament of suddenly trans-identifying teens.” This is disingenuous on at least two levels: the conversations around care of trans youth have historically centered on parents, and there is an abundance of “lone sympathizers.”
None of the parents interviewed accurately gendered their children. In one instance, the parents wanted assurance that their child’s school would treat their child as a girl and use the “given name and female pronouns.” One family moved across country to re-immerse their child in traditional Indian culture. A youth refused to come home unless their parents permitted them to stay on testosterone. The parents stated, “we wouldn’t pay for (her) heroin.”
The parents sought out alternatives to gender affirming therapists. One pair accepted their child as lesbian but coming out as trans was “a bridge too far.” A father characterized his child thusly: “(she) thinks (she) looks like a guy. (She’s) got the hair on (her) arms and everything, but (she’s) beautiful. They were actually calling (her) ‘sir’ on our vacation, which was crazy. To me, (she) doesn’t look like anything but my (daughter).” Both parents of the youth see their child’s gender identity as a “problem.”
One parent, speaking of their child, reports: “all (her) friends are bisexual. There’s only one heterosexual girl in (her) little crew. Everyone else is lesbian, bisexual. My (daughter) had to one-up them and be ‘trans.'” One youth, post-top surgery and “covered in tattoos,” was persuaded by their mom that “transgender shouldn’t be on (their) resume.” A father told their child to consider “appearing a little less unusual” while job-hunting. A mother regretted being “indulgent of her (child’s) gender exploration”; regretted not telling them coming out as trans at 12 years old was ridiculous. She concluded that she should have been less open to listening to her child.
Shrier summarizes: “there’s nothing crueler, more “toxic” to trans gurus than parents who fail to jump on board with each step of gender transition and every tenet of gender ideology.” The parents are the true victims here, “Even if they can’t seem to quit that birth name they dumbly believed they had the right to give you just because every parents since the beginning of time assumed the same” and “don’t know the difference between genderqueer and transgender no matter how many times you explain it” and “may never see you as the sex you wish to be.”
Their trans children are the toxic ones, turning their anger on those who least deserve it.
The rates of suicidality, depression, anxiety, low self-esteem, self-harm, and substance use in trans youth increase proportionally to increased levels of family rejection. The Trans Pulse Project, a community-based, mixed-method research project, reported that 57% of trans youth without parental support endorsed a suicide attempt in the past year, compared to 4% of those supported. Most recently, the National Survey on LGBTQ Youth Mental Health 2021 gathered data from 34,759 U.S. LGBTQ youth aged 13-24. Only 1 in 3 found their home to be affirming and 80% stated that COVID-19 made their living situation more stressful. Trans youth who did not have their pronouns respected by all the people they lived with attempted suicide twice as much as those whose pronouns were respected. Those not permitted to change legal documents to match their gender identity attempted suicide over twice as much compared to those who changed their documents.
Positive family relationships are broadly protective for trans youth; family rejection is one of the biggest predictors of suicidality. Trans children supported in their gender identity by their families have rates of depression comparable to their cisgender peers. Studies suggest that improved body satisfaction and self-esteem following the receipt of gender-affirming care is protective against poorer mental health and supports healthy relationships with parents and peers. Research consistently demonstrates that trans youth who are affirmed in their gender identity by their families have significantly better health outcomes. There is a need for larger-scale studies that include questions about gender identity, notably absent in prior research, recruitment in rural areas as well as metropolitan, inclusion of intersectional minorities overlooked and ignored by the system, and analysis of the specific factors that predict rejecting family behaviors and those that contribute to positive climates.
“The Trans Agenda,” part 6: Deny biology
Shrier writes that being gay is innate, biologically determined, and immutable. She notes that being trans is not like being gay; she asserts, “we know that homosexuality can’t be eliminated through socialization” but “we don’t have any similar weight of history telling us that we can’t treat gender dysphoria.”
Interesting how the tide turns, as homosexuality was pathologized by medicine for decades.
In 1952, the first edition of the DSM listed homosexuality as a sociopathic personality disturbance. In 1974, homosexuality as a disorder was removed, and the diagnosis was changed to “sexual orientation disturbance.” The 1980 DSM-III replaced this diagnosis with “ego-dystonic homosexuality,” and added the new diagnosis “gender identity disorder.” In 1987, the DSM-III-R replaced “ego-dystonic homosexuality” with “sexual disorder not otherwise specified,” a diagnosis that included “persistent and marked distress” about one’s sexual orientation.
The same arguments for removal of gender dysphoria from the DSM-V were debated around the DSM-II diagnosis of homosexuality: societal discrimination, the stigma of a mental health diagnosis, the psychopathological framing of normal variations in expression and identity and focusing psychiatric attention on individuals instead of on opposing the forces that oppress sexual and gender minorities. Gender identity, whether trans or cis, should need no justification or explanation; that said, decades of research support a significant biological contribution to the development of sexual orientation and gender identity.
Shrier seems to see trans people through a disease framework: being trans is the delusion of someone with a mental illness. To Shrier, gender is not self-determined; trans adults are those who “present as women and present as men,” and nonbinary people are “neither”, an “in-between state” with “indeterminate and shifting goals.” One trans YouTuber is characterized by Shrier as “still obviously female but trans-identifying,” and she mocks him for “shrieking” when he gets his first binder: “breasts may be painful reminders of one’s birth sex, but apparently shrieking is not.” Shrier’s personal assessments of trans people are to her undeniable proof of a biological reality.
Gender identity education in schools, says Shrier, is “gibberish” and “drivel:” “It is biologically impossible to suggest that a girl’s brain-every cell of it stamped with XX chromosomes-might inhabit a boy’s body.”
In Shrier’s line of thinking, individuals are either born with two XX chromosomes, a vagina, ovaries, and uterus, produce high levels of estrogen, and carry children, or born with an X and a Y chromosome, penis and testicles, produce high levels of testosterone, and father children. Setting aside Shrier’s gender essentialism and the facts that sex is not gender and sex is not binary, middle school textbooks may teach that XX chromosomes mean female and XY chromosomes mean male, but biology is much more complicated.
Qualifying brains as “male” or “female” is overly simplistic (and biologically impossible.) Though there are sexually dimorphic characteristics, brains do not align to the male/female binary. As Cognitive Neuroscientist Gina Rippon notes, “a gendered world will produce a gendered brain.”
Complex genetic signals can lead to, for example, an AMAB person having XX chromosomes, and an AFAB person being XY. There are a number of other sex chromosome abnormalities. The cluster of cells that forms the bipotential primordium in a fetus can turn into testes, ovaries, or neither. Genes that maintain certain sexual characteristics in adulthood can stop working, causing gonads to change in appearance. We associate estrogen and progesterone with AFAB people and testosterone with AMAB people, although both AFAB and AMAB people have them, and levels can fluctuate wildly between individuals. Environmental, social and behavioral factors all influence hormone levels in adults.
There are various differences in sex development, or DSD. Some use intersex, as the term DSD implies they need to be fixed, although others argue that the term intersex implies sexuality, which is unrelated. Terminology is complicated and ever-shifting; it is not for those outside of the community to decide which terms should be used. In the 1950s, Johns Hopkins Surgeon Dr. John Money’s research on intersex individuals and genital reassignment surgery led him to theorize that gender is malleable, its development predominately dependent on external/environmental factors. This encouraged the surgical practice of “normalizing” those with variations in sex characteristics. Framing the estimated 1.5 to 2% of the population born with non-binary genitalia as disordered justifies pathologizing and “correcting” healthy bodies with nonconsensual surgical interventions, a practice common to this day.
Shrier relates the story of David Reimer, an individual born with XY chromosomes who, after a botched circumcision, was surgically assigned female. Dr. Money claimed success with his patient, who was raised as a girl. This is evidence that gender is learned, he asserted. But from a young age, David did not identify as a girl; he was bullied and developed suicidal depression. Eventually David got surgery to reverse the damage done to him. After years of emotional turmoil, he committed suicide at age 38.
David Reimer’s tragic story is Shrier’s proof that sex assigned at birth and gender identity are the same, and that David could not “escape” his “biology.” David’s penis and testicles were removed, halting the development of male sex characteristics, and he still did not express a female gender identity. His own body was telling him he was female, but he asserted a male identity. The body does not determine gender. Doctors and parents cannot choose a person’s gender identity.
Two other important points:
- David was not trans. His genitalia prior to being surgically altered were aligned to his asserted gender identity. Being intersex and having your genitalia coercively sexed is different from being assigned a sex at birth that is discordant with your identity.
- In her argument for biological inevitability, Shrier is likely unaware that Money believed gender identity to be fixed by about 4 ½ years old and efforts to change a person’s gender identity after this age were nearly impossible.
“The Trans Agenda” part 7: Gender affirmation for all!
Shrier asks, “do we have any evidence that affirmation ameliorates mental health problems?” Her answer is no. The “current (transgender) craze is so new,” says Shrier, that there are no definitive studies addressing mental health.
Social and medical gender affirmation are inversely related to mental health problems in trans people. Research overwhelmingly supports an affirmative approach.
Social affirmation
Trans youth often (but not always) start exploring their identities within the social affirmation model. Social affirmation can include using a chosen name, changing one’s hairstyle and/or clothing, using aligned pronouns, packing or tucking, binding, changing legal documents to reflect chosen name and gender identity, and coming out. Care is tailored to the youth and their families in order to create a safe and supportive environment. The model seeks to destigmatize trans identity, promote the child’s self-worth, educate family members, and facilitate access to care and community spaces. Social affirmation is entirely reversible and makes the youth feel supported. Observational data supports that intense gender dysphoria, moods, and behavior improve with social affirmation. Those allowed to use their chosen name are less depressed and suicidal. 13 other studies report at least one significant association between social affirmation and mental health outcomes.
Shrier believes that a child should not be affirmed in their self-reported gender identity, because this may cause that identity to “harden…in the child’s mind” and cause confusion. The manual that Shrier cites here is described by the Human Rights Campaign (HRC) website as:
[A] groundbreaking guide, written for administrators, teachers, parents, and other adults who work with youth, covering topics ranging from basic concepts of gender and the importance of affirming gender identity, to best practices for restroom access and working with unsupportive parents.
A gender-expansive student should never be asked, encouraged or required to affirm a gender identity or to express their gender in a manner that is not consistent with their self- identification or expression. Any such attempts or requests are unethical and will likely cause significant emotional harm. It is irrelevant whether a person’s objection to a student’s identity or expression is based on sincerely held religious beliefs or the belief that the student lacks capacity or ability to assert their gender identity or expression (e.g., due to age, developmental disability or intellectual disability).
The consequences of not affirming a child’s gender identity can be severe, and it can interfere with their ability to develop and maintain healthy interpersonal relationships. In the school context, that distress will also hinder a transgender student’s focus in class and ability to learn. The longer a transgender youth is not affirmed, the more significant and long-lasting the negative consequences can become, including loss of interest in school, heightened risk for alcohol and drug use, poor mental health and suicide. [Bolding mine – AJE]
Trans identity drives social affirmation rather than being a consequence of it. A recent study shows that trans youth still living as their sex assigned at birth are as strong in their gender identity as those who are living as their gender identity. A trans boy still living as a girl and a trans boy affirmed to live as a boy both know their gender identity; the boy affirmed in his gender does not just feel or act like a boy because he is being treated like a boy. Research concludes that most likely trans identity exist prior to-and not because of-social affirmation.
The risks of social affirmation are the risks of a transphobic culture: discrimination, oppression, ostracization, stigma, loss of extended family support, and rejection from the outside world. The risks of not socially affirming include higher rates of depression, self-harm, suicidality, anxiety, and eating disorders; once puberty hits, add to these substance use, PTSD, risky behaviors and minority stress.
The oft-repeated claim that social affirmation makes it harder for children to return to their assumed gender identity is drawn from one study which discusses examples of “persisters” and “desisters.” The study is a qualitative follow-up on children seen at the Amsterdam Gender Identity Clinic from 2000-2007. 25 adolescents were interviewed.
- Desister #1: “always accepted by boys,” frequently asked by others if she was a boy,
- Desister #2: “knew very well” that she was a girl “who wished to be a boy”.
Neither “desister” noted body discomfort and feelings of misalignment, which all “persisters” expressed. Both expressed the “wish” for another body in order to fulfill the desired social role. For all “desisters” gender discomfort gradually decreased and disappeared with physical pubertal changes. They all reported continued “gender atypical interests” and “significant feelings of shame” for their earlier “boyish appearance.”
The study notes, “none of the girls ‘officially’ transitioned by changing their name or informing other children that they wanted to be referred to as ‘he.'” This is not social affirmation. These girls were tomboys with “boyish” haircuts and clothing. They were perceived as boys as a result of their appearance and behavior. Gender expression is not gender identity. Wanting to be a boy but knowing you’re a girl is different from being AFAB and knowing you’re a boy. The study used the DSM-IV definition of gender identity disorder for the children, which does not distinguish between “gender variant expression” and gender dysphoria.
These are not trans children with gender dysphoria. This is not social gender affirmation.
Still, the researchers conclude that a cautious attitude should inform clinical management of children under the age of 10 and warn of the difficulties of a transitioned child wanting to revert to their original gender role.
This study informs the knowledge base on trans youth and is cited in subsequent research studies. This sentence needs to be longer to link more of these studies.
Binders
Shrier writes that binders (which she pointedly refers to as “breast binders“) cause “dangerous medical side effects,” such as fractured or bruised ribs, punctured or collapsed lungs, shortness of breath, back pain, and deformation of breast tissue. Shrier sources a Vice article, characteristically cherry-picking. The same article reports that chest binding for many trans people is a matter of psychological well-being, and helpful in reducing gender dysphoria. The true danger with binding is that healthcare professionals are largely unaware of the phenomenon and need to be educated on how to help people bind safely and effectively.
The first study on chest binding was published in 2016 and noted that binding is a positive experience for most, leading to improvements in mood, self-esteem, anxiety, and depression. Most common side effects are back pain, overheating, chest pain, shortness of breath, itching, bad posture, and shoulder pain. Despite these health concerns, most people still bind, due to the positive effects on mental health and quality of life. Rare but serious outcomes, such as rib fractures, take years to occur. Symptoms are minimized or prevented with proper education and guidance. Access to puberty blockers delays the initiation of binding, reducing side effects in youth.
Mental health
To understand the gender affirmative approach, we need to review two other approaches to therapy for trans youth: conversion and watchful waiting.
The conversion approach
Conversion therapy is any attempt to change a person’s sexual orientation, gender identity, or gender expression. Due to the increased scrutiny around this practice, it is known under various aliases: Sexual Orientation/Gender Identity Change Efforts (SOCE/GICE), Sexual Attraction Fluidity Exploration in Therapy (SAFE-T), eliminating, reducing or decreasing frequency or intensity of unwanted Same-Sex Attraction (SSA), reparative therapy, sexual reorientation efforts, ex-gay ministry, promoting healthy sexuality, addressing sexual addictions and disorders, sexuality counseling, encouraging relational and sexual wholeness, healing sexual brokenness, reorientation therapy, reintegrative therapy.
Conversion therapy is a discredited, unethical, pseudoscientific practice grounded in the belief that sexual and gender minorities are deviances that need to be corrected. In the conversion model, being trans is an undesirable pathology and gender identity is seen as malleable, as long as the child is treated early. Many clinicians still practice this approach, despite the medical consensus of more than 40 professional regulating bodies that trans identity is not negative or pathological. The HRC published an extensive list of the major medical organizations that support a conversion therapy ban.
A 2019 study reports that almost 200,000 trans people in the U.S. have been exposed to conversion therapy in their lifetime. When LGBQ people are included in this statistic, the number goes up to 698,000. The Trevor Project’s 2020 National Survey on LGBTQ Youth Mental Health, representing over 40,000 LGBTQ youth aged 13-24 across the U.S., reports that 6 out of 10 LGBTQ youth said that someone tried to convince them to change their gender identity or sexual orientation. Those who were directly exposed to conversion therapy had a 28% suicide attempt rate, vs 12% for those not exposed. Most of them had undergone conversion therapy as minors.
Conversion therapy has been associated with internalization of stigma and discrimination, self-harm, poor self-esteem, self-hatred, depression, anxiety and substance use. There is no federal ban on conversion therapy, so the practice continues across the United States, especially in religious communities who are exempt from any state legislation. Only 20 states have bans on conversion therapy; in those states, a loophole is practicing conversion therapy outside of professional associations, meaning practicing without a relevant degree, certification, or license. Some say conversion therapy bans are a violation of free speech.
The “watchful waiting” approach
First described in 1998, the watchful waiting approach was designed to treat “carefully identified patients” with puberty blockers at 12 years old, and gender affirming hormones at 16 years old. Also known as The Dutch Protocol, or The Dutch model, this cautious approach is informed by the belief that most children with gender dysphoria desist before adolescence. That belief is based in flawed and biased research, and negates those trans children with an asserted and clear gender identity, since they are not to be trusted until an arbitrary point in adolescence. In this schema, social affirmation may be unnecessary or even harmful, and certain forms of gender expression are prohibited until the child is older. Access to affirmation is based on the child’s age.
Though Shrier supports watchful waiting, she is against the use of puberty blockers. She believes that watchful waiting “help(s) a child grow more comfortable in his or her biological sex,” and claims that this approach has been “remarkably successful.” Shrier defends those health professionals who “could be accused of trying to “convert” their patients out of a transgender identity” in their practice.
We trust cisgender children to manage and assert their gender identities; why don’t we trust transgender children (when the medical consensus is that trans identities are as equally valid as cis identities)?
The gender affirmative approach
To Shrier, the gender affirmative approach means there are no safeguards for treatment. “The dangers are legion,” she warns.
The gender affirmative approach places significance on a child’s understanding of their own gender and supports trans children in gender affirmation, reassuring them that there is nothing wrong with their gender identity or expression. This approach can alleviate mental health and behavioral concerns in a trans child. As discussed, family support is vital to a child’s well-being, and in a gender affirmative approach, healthcare professionals collaborate with children and their families to create individualized affirmative frameworks. Therapy is not a requirement in this approach because being trans is not a pathology.
As Developmental and Clinical Psychologist and prolific researcher in the field of childhood gender identity Dr. Diane Ehrensaft writes, “from the gender affirmative perspective, authenticity leads to connection, security, attachment, empowerment, and overall well-being whether you are 5, 14, or 50 years old.”
Medical affirmation
Puberty blockers
Puberty begins when the hypothalamus in the brain starts producing gonadotropin-releasing hormone (GnRH). GnRH activates the anterior pituitary gland, releasing gonadotropins (leutinizing hormone, LH, and follicle-stimulating hormone, FSH) that cause gonad maturation. This leads to the production of sex hormones in the testes and ovaries. Puberty blockers stop the release of gonadotropins from the pituitary gland which stops production of sex hormones. Agents used include leuprolide acetate, histrelin acetate, and triptorelin pamoate. Shrier opposes the idea that puberty blockers as a “pause button,” but that is an accurate characterization: once blockers are discontinued, sex hormone production resumes. Puberty blockers are safe, effective, and reversible.
Gender dysphoria in trans youth is often triggered by or worsened with onset of pubertal changes. Blockers stop the development of secondary sexual characteristics, including penis growth, Adam’s apple development, voice deepening, and tall stature in AMAB youth, and breast development, periods, and short height in AFAB youth. Puberty blockers give the youth and their family time to explore their gender identity, halt changes that can lead to difficulty “passing” for binary trans people and reduce the need for future surgeries. Puberty can be extremely traumatic for trans youth and is irreversible; waiting to see if gender dysphoria resolves is not a neutral response.
Puberty blockers have been used to delay puberty since 1981, with 30 years of follow-up data showing they are safe and effective. The most common side effects of blockers, according to a critical review of the literature, are fatigue, mood swings, and hot flashes in initial phases of treatment. Symptoms are minor and diminish over time; it is rare for youth to discontinue blockers due to side effects. Long-term follow-up studies have shown that AFAB people with central precocious puberty treated with blockers have normal BMI, BMD, body composition, and ovarian function in early adulthood, with no evidence of predisposition to PCOS or menstrual issues, and no other longterm adverse effects. Gender-affirming medical interventions such as puberty blockers are indicated once a youth starts showing signs of puberty (Tanner stage II development.)
To Shrier, puberty blockers are “chemical castrator(s),” “medications that induce chemical menopause to artificially halt puberty.” She states that there are no reliable studies to support that Lupron is safe for trans youth. The side effects of blockers, according to Shrier, include suppression of normal bone density development, greater risk of osteoporosis, loss of sexual function, interference with brain development, and possible suppression of peak IQ. Writes Shrier, the side effects of blockers “dramatically increase if an adolescent moves straight from puberty blockers to cross-sex hormones.” Infertility is almost guaranteed, she warns. Sexual development and potential for orgasm “may be foreclosed for good.” A “girl” on blockers will “feel more alienated from womanhood, not less,” which is, concludes Shrier, why “she” will proceed to taking gender affirming hormones.
Puberty blockers as chemical castrators are a favorite conservative talking point.
And yes puberty blockers are chemical castration. It's the same drug they use to chemically castrate sex offenders. Yes this is shocking and hard to believe but it's also true. This is the world we live in now. Wake up and start paying attention.
— Matt Walsh (@MattWalshBlog) October 24, 2019
The same medications, formulations, and even doses are used to treat prostate cancer, endometriosis, precocious puberty, and infertility. For decades, cis children with central precocious puberty have been treated with puberty blockers with exactly zero concerns raised about chemical castration or “alienating” cis youth “from womanhood.” Puberty blockers are not FDA-approved for trans youth, but this does not make them experimental or unstudied. Blockers have been used as treatment for dysphoric trans youth since the 1990s. Off-label drug use, or prescribing medications for indications not approved by the US Food and Drug Administration, is incredibly common in every specialty of medicine; the FDA does not regulate the practice of medicine. Off-label drug use can become a widely accepted practice and even standard of care.
A 2019 retrospective review of trans youth on blockers noted no significant change on bone mineral density over 3 years of DEXA bone scans. Z-scores (a measure of bone mineral density) decreased as expected, but the relevance of these findings with respect to fracture is unclear. BMD and Z-scores increase after the addition of hormones. A cross-sectional analysis of the longitudinal, observational, prospective Trans Youth Care Study cohort notes a high prevalence of low BMD in early pubertal trans youth before starting hormone blockers, which is consistent with prior studies. It is important to note that earlier studies reporting low bone density in trans youth were comparing trans youth on blockers to same-aged cis youth in puberty. Puberty causes an increase in bone density. Blocking puberty will then, naturally, halt this increase; therefore, bone density will decrease in these trans youth compared to cis youth, an expected result. Those on blockers who postpone gender affirming hormones may be particularly prone to loss of bone mass, as BMD and bone mass are inversely related to the timing of puberty. Trans youth treated with puberty blockers in early puberty have changes in bone health comparable to those of cis youth of their experienced gender. The Trans Youth Care cohort will follow the trajectory of bone mineral accrual for trans youth treated with puberty blockers and then hormones; research is forthcoming.
Studies on brain development have found no significant differences in youth on blockers. Puberty blockers do not have a detrimental effect on executive function. A longitudinal study found that trans youth on blockers have significantly better global functioning than those not on blockers.
Shrier’s most lamented side effect of gender affirmation is “sterility.” These medications, says Shrier, claim fertility for good, “eliminating…a vital human capacity.” Since blockers only temporarily suppress sperm and ova maturation, they have no effect on future fertility. If a youth on blockers begins treatment with gender affirming hormones, ova and sperm will not mature for menarche or spermatogenesis to occur. One case study reported successful oocyte cryopreservation in a youth who had been treated with blockers and hormones. A NEJM correspondence discusses a youth who underwent cryopreservation while on blockers. Given the paucity of research and a range of fertility desires, healthcare providers should discuss fertility and reproductive health with trans youth and their families prior to any gender affirming treatment. Barriers include inadequate provider knowledge and training, inconsistent fertility counseling, high costs of treatment, and difficulty considering future parenthood in the context of gender dysphoria distress. Oocyte cryopreservation, the only established option for fertility preservation in trans youth, is invasive, expensive, and time-consuming, and may cause severe discomfort and worsening of gender dysphoria. Even with fertility counseling, rates of fertility preservation are low, with many expressing a desire to adopt or not wanting children in the future.
There are many opinion pieces that reflect Shrier’s concern about negative effects puberty blockers have on trans sex lives and orgasms. The lack of evidence to support this concern is unimportant to many adults online speculating about trans youth sex lives. The evidence bandied around: a study on erectile function in patients with prostate cancer on blockers; an interview with Jazz Jennings misrepresenting her statements; speculation around bottom surgery outcomes and genital development. Many youth with gender dysphoria are uncomfortable with their genitals; a lack of sex life does not indicate poor sexual functioning. Shrier wonders whether “becoming” trans is “all an act of sexual withdrawal and avoidance.”
Cisgender people do not and cannot understand the dimensions of trans sexuality. I would posit that it is not for them to understand. Until they can support their concerns with evidence-based research, the gross speculation needs to stay out of trans peoples’ bedrooms. But to alleviate Shrier’s worries: a 2020 study on youth who were affirmed with blockers, then hormones and surgery noted a significant increase in sexual experiences one year post-surgery.
Shrier interviews endocrinologist Dr. William Malone, an “outspoken critic,” who views the use of blockers in trans youth as “an intervention that halts normal, healthy biological functioning…introducing the “disease state” brought on by a pituitary tumor-all based on self-reported mental distress.” To Malone, no child is born in the wrong body.
A claim espoused by Zucker and endorsed by Shrier is that studies show “that nearly all adolescents who identify as transgender and are put on puberty blockers go on to take cross-sex hormones in adulthood.” This is an extension of the social affirmation argument: affirming a youth’s gender identity causes that youth to double down on that identity, helping youth “impersonate the opposite sex.”
Yes, many trans youth start gender affirming hormones. Trans adolescents know who they are. Those youth who started on blockers and move on to gender-affirming hormones do so because they are trans.
Moreover, trans youth do not have the easy access to blockers that Shrier portrays; there are many barriers to gender affirming care. Trans youth depend on their families for medical decision-making, and may be unable to access treatment due to anti-trans medical care bans, harassment, refusal of care, lack of support, cost of medications, spotty insurance coverage, fear of doctor attitudes, lack of options, and long clinic waiting periods, leading to delays in timely care. Clinics may be far and trans-competent providers are few and far between. Access is disproportionately limited for low-income trans people and communities of color. Nonbinary youth face the additional challenge of accessing trans healthcare that follows the traditional binary model. Obtaining competent health services is historically challenging for trans youth and not much has changed.
Research supports that the mental health benefits of puberty blocker treatment outweigh any potential side effects of blockers. There is a significant inverse relationship between puberty blocker gender affirmation and lifetime suicidal ideation. Major medical organizations including the APA (American Psychiatric Association) endorse the use of puberty blockers and oppose legislative and governmental attempts to limit access to blockers for trans youth.
Testosterone
The most common gender affirming hormone treatment for AFAB trans people is testosterone. Testosterone use under the supervision of a healthcare provider is safe, based on both short-term and long-term studies. Testosterone causes virilizing effects on the body, such as increased facial and body hair, voice deepening, and period cessation. Testosterone also reduces gender dysphoria, anxiety, and depression.
According to Shrier, testosterone is freely dispensed to “girls with no history of dysphoria,” who are set on a path to a “lifetime of hormone dependency and disfiguring surgeries.” What a high price to pay, she notes. Shrier reports that adolescents believe that “T”, a colloquialism for testosterone in the trans community, will solve all problems. She extrapolates this from testimonials of happy trans people on testosterone, neglecting to take into account the catharsis and gender euphoria of finally being able to affirm one’s gender identity.
Testosterone may not solve all problems (and no one claims it would), but medical affirmation can be a giant step toward improving quality of life and diminishing depression and anxiety. Shrier’s take is that AFAB teens are “self-medicating” and calling their distress gender dysphoria, when it may in fact be anxiety and depression. To understand this take it may be useful to define gender dysphoria.
The World Professional Association for Transgender Health Standards of Care describe gender dysphoria as distress caused by a discrepancy between a person’s gender identity and their sex assigned at birth. Since the diagnosis of gender dysphoria appears in the DSM-V, many people still wrongly insist that trans people are mentally ill. Dysphoric feelings about one’s primary and secondary sex characteristics, being labeled as “the wrong gender,” and societal prejudice, social norms, and stigma may lead to psychiatric symptoms in a trans person. Gender identity in itself is not a mental illness. Prior research attempting to measure gender dysphoria has severe methodological flaws; a 2021 systematic review recommends not using any previous measures for future study without further development. Flaws are understandable given the evolution of the medical definition of gender dysphoria, however, many researchers continue to use outdated measures.
To sum: gender dysphoria is not anxiety and depression. Gender minority status, often compounded by gender dysphoria, can lead to anxiety and depression.
Trans youth consider the “health risks” of T a perk, according to Shrier. “If you want to become a man, you have to expect being strong like one, horny like one, and, yes, prone to a heart attack like one.”
Well, yes. I would note that strength and libido are not health risks. Testosterone use likely does increase cardiovascular risk, with expected results: trans men on T have an increased risk when compared to cis women; the risk for trans men is equal to that of cis men. There is no increased morbidity or mortality in trans men in short- and medium-term studies. Research has demonstrated that testosterone-driven increases in hematocrit, triglycerides and LDL do not lead to significant increases in cardiovascular outcomes or lead to adverse cardiovascular outcomes. Data on transmasculine people over 65 years old is lacking.
Shrier mentions blood thickening. Testosterone can sometimes cause secondary polycythemia, or erythrocytosis, an increase in red blood cells that causes thickening of the blood. Though this phenomenon has been noted in several studies, there have been no reported thromboembolic events. This follows, as primary polycythemia is associated with increased thrombotic risk, but not secondary polycythemia. In a clinical setting, healthcare professionals minimize side effects by monitoring transmasculine people on testosterone with periodic bloodwork, including a hematocrit. If erythrocytosis is noted on labs, healthcare professionals may consider changing route of administration or decreasing testosterone dosage, despite absence of outcome data showing risk reduction of thrombotic events.
Shrier states that testosterone levels in AFAB transmasculine youth are 10-40 times higher than those of cisgender AFAB youth. Bearing in mind the wide variability of testosterone levels, “normal” levels for AMAB adolescents (15 and above) are 100-1,200; “normal” levels for AFAB adolescents (15 and above) are 7-75. Target ranges for testosterone treatment in AFAB trans youth are physiologic cisgender AMAB ranges. Clearly, the ranges are wide; if we take a mean of both numbers, the levels are about 16 times higher for those on testosterone (but that’s the point.)
Testosterone use causes “increased risks of various cancers”, Shrier gestures vaguely, and this risk will lead to an eventual “prophylactic hysterectomy.” An increased prevalence of cancer in trans men is not supported by existing evidence. Testosterone does not seem to increase the risk of breast, cervical, endometrial, ovarian, or uterine cancers. A retrospective multicenter case series noted an active endometrium in most patients on testosterone and no cases of endometrial cancer, despite amenorrhea. A histologic analysis of specimens from 112 patients who underwent total abdominal hysterectomy with bilateral salphingo-oophrectomy noted no evidence of cancer or premalignant changes.
Missing a dose of T, according to Shrier, increases the risk of cell mutation and endometrial cancer. Citation needed; this is not a thing.
Current guidelines suggest conducting routine cancer screening based on anatomical inventory (organs present). The overall base of research into cancer and trans people is small, and more research is acutely needed, including evaluation of the constraints that may limit trans patients from seeking preventive screening examinations, and correlation of findings with smoking, substance use, STIs, and lack of screening. More research is upcoming.
Shrier warns, “they (trans teens) extol the glories of testosterone as if it were a protein shake, not a Schedule III controlled substance.” If Shrier was truly concerned about the dangers of testosterone, she might mention its decades-long rampant abuse among cisgender men. Anabolic steroids are synthetic derivatives of testosterone used for doping to improve athletic performance. This is a practice banned in most sports; widespread anabolic steroid abuse and subsequent sports scandals led to the 1990 Anabolic Steroid Control Act, in which Congress designated testosterone as a “controlled substance.” Another common misuse of testosterone is supplementing low testosterone levels caused by aging, marketed in the 2000s as “andropause,” a made up and discredited diagnosis. The “protein shake” analogy seems a deliberate attempt to draw a parallel to athletes and doping. The comparison is lacking, as the dosage of anabolic steroid use to enhance performance is anywhere from twice as high as doses in gender affirming treatment to 40 times higher than therapeutic testosterone doses.
According to Shrier, “if you’re up for something really edgy, there’s (also) the self-administered intramuscular shot,” a strange statement, since testosterone injections are the most commonly used method. Is that edgy?
Shrier warns of sexual side effects of testosterone, but the research she cites does not support her stance the way she thinks it does. The study is clear that sexual dysfunctions experienced by trans people, namely difficulties initiating and seeking sexual contact and difficulties achieving orgasm, are greatly influenced by potential social and psychological barriers.
Permanent changes on testosterone, according to Shrier, include extra body and facial hair, deepened voice, clitoral enlargement, and masculinization of facial features. Some of the effects of testosterone treatment are reversible if a person stops taking testosterone. Voice changes, clitoral enlargement (bottom growth), and facial hair growth are permanent. Body and facial hair may regress; masculinization of facial features and fat redistribution will revert based on length of time on hormones/length of time off hormones.
Voice change is, for many, one of the most important effects of gender affirmation. Testosterone treatment has a positive effect on body image. Testosterone reduces unease around the body, dissatisfaction with body parts, and sexual distress.
Per Shrier, “providers happily serve(d) up puberty blockers and courses of testosterone.”
‘The moment these girls voice the shibboleth “I’m trans,” nearly every adult, even medical professionals, regard them with the awe owed to a prophet.’
Who? Where?
The vast majority of trans youth in the U.S. lack access to competent, responsible, and affordable care. Although there has been a move in recent years to an informed consent model of gender care to replace the traditional gatekeeping models, access to care is difficult for people living outside of major metropolitan areas. Trans youth face both individual and systemic barriers to health care. The biggest barrier is a lack of knowledgeable providers, followed by discrimination and lack of cultural competence by providers. The 2015 U.S. Transgender Survey found that nearly 25% of trans people avoided seeking healthcare in the past year due to fear of discrimination or mistreatment based on gender identity. 55% of insured respondents surveyed by the 2015 U.S. Transgender Survey report being denied coverage for gender-affirming surgery. Some states have no LGBT community health centers. Electronic medical records often fail to identify trans patients. The LGBTQ population remains underserved and ill-served by the healthcare system.
Surgical gender affirmation
Shrier hits on a salient point when she writes, “one prominent microsurgeon at one of the premier hospitals in the country told me that gender surgeries are such moneymakers, his hospital hires doctors to do gender surgeries who, in his opinion, are not qualified for the work.” This is sobering. Surgeons are not formally trained to perform gender affirming procedures, and there is no parameter to ensure they are adequately experienced to do these surgeries. The average plastic surgery medical resident received at most 18 hours of trans health education in 6 years of training. This is universal in medical education as trans healthcare is not mandated in medical school and residency curricula. Hospitals lack trans policies and healthcare provider attitudes toward trans patients show bias and lack of knowledge. There are limited programs offering gender affirmation surgery. It is difficult to confirm whether a surgeon who lists gender affirming surgery on their profile performs these procedures and/or performs them well.
Top surgery, a colloquialism for bilateral chest masculinization surgery, is the most common gender affirmation surgical procedure for transmasculine people. Top surgery is generally more important for AFAB trans people than other gender affirming surgeries because of outward gender expression: the presence or absence of breast tissue is readily visible to others in daily life. Unlike estrogen-based hormone treatment for transfeminine people which causes breast development, testosterone does not significantly affect chest size.
Top surgery is an elective procedure that “destroys biological capacity,” writes Shrier; a “voluntary double mastectomy” pushed on trans people by a “monstrous ideology.” She compares the desire for top surgery to her own desire for a breast reduction when she was young. How could she trust her desires when, over a decade later, she had nursed 3 children? Shrier characterizes AFAB trans youth as cavalier risk-takers, cheered on by their friends. Any desires they have should be met with skepticism.
Shrier sources the 2017 Plastic Surgery Statistics Report to note that from 2016 to 2017, AFAB people accounted for 70% of all gender surgeries. The statistic reflects procedures performed by board-certified members of the American Society of Plastic Surgeons, an organization that only began tracking these procedures around 2016. The report lumps the many different procedures for gender affirmation together into one statistic, divided by sex assigned at birth. The mean age for AFAB chest surgery is 28.6 years old; I am unclear why the 70% statistic is even included in a book on transgender youth.
70% is a high number, meant to elicit concern about the prevalence of gender affirming surgery for AFAB trans people.
Says McHugh, “the problem with gender surgery is that doctors have no way of knowing who will be healed and who will be harmed by it” and there’s no way to tell the difference between those who will and won’t regret it. This is just not true.
Suicidality goes up after gender affirming surgery, asserts Shrier, noting the Karolinska Institute study. The study followed 324 Swedish trans people who had gender affirming surgery between 1973 and 2003 and reported a higher suicide rate in trans people post-transition compared to the general population. This source is heavily cited to support the claim that gender affirmation does not work and, in fact, causes more distress for trans people. McHugh is a fan; he characterizes the study as yielding the “most illuminating results yet regarding the transgendered.”
The Karolinska study actually states “the results should not be interpreted such as sex reassignment per se increases morbidity and mortality. Things might have been even worse without sex reassignment.” The study did not address whether sex reassignment is an effective treatment or not. It also did not assess suicidal ideation prior to gender-affirming surgery. Lead researcher of the Karolinska study, Dr. Cecilia Dhejne, says her study was misrepresented. In an interview with TransAdvocate, she remarked, “of course trans medical and psychological care is efficacious.”
Another oft-cited study is a 2020 paper on the Amsterdam Cohort of Gender Dysphoria (1972-2017). The study noted a risk of suicide 3 to 4 times higher in trans people compared to cis people, which did not change (but also did not increase) with gender affirmative treatment and even decreased over time in trans women. Similar to the Karolinska study, this research was interpreted by Shrier and co. as proof that gender affirmation does not work. The study researchers noted that suicidal behavior is complex, and cited a recent literature review that “clearly demonstrates the specific risk factors for suicide in sexual minority youth, which includes negative social environments, inadequate support within the closest social network, and an absence of lesbian, gay, bisexual, and transgender (LGBT) movements in communities.” The study recommends that future research should focus on suicide risk factors in trans people and concludes that it is important for healthcare professionals to create a safe environment and pay attention to risks.
Long-term outcome data from the Netherlands on trans people treated with pubertal suppression followed by hormones and finally gender affirmation surgery yielded positive outcomes and no one regretted starting gender affirming medical treatments. In a study primarily sampling participants from the United States, AFAB trans individuals reported a diminished quality of life compared with cisgender males and females; however, those who had received testosterone reported significantly higher quality of life compared with those who had not. A review of 29 academic studies found a very high rate of satisfaction among phalloplasty patients. A systematic literature review of all peer-reviewed articles about the relationship between gender transition and mental health published in English between 1991 and 2017, noted that overall well-being of trans people improves with gender affirmation. Gender affirming healthcare is not only effective but medically necessary for those who seek it and associated with improved mental health and decreased gender dysphoria. Gender affirming surgery needs to be more accessible in order to develop optimal evidence-based guidelines for the health of trans individuals. Further research is necessary to keep up with the healthcare needs of the trans population.
“Detransitioners” and “desisters”
Perhaps one of the most common narratives of those who oppose gender affirming care is the one centered around “detransitioners.” The media consensus: “Trans healthcare is dangerous and harmful! Look at all these people who regret this giant mistake.” The rhetoric around “detransitioners” is not dissimilar to that of the “ex-gay” movement, both insisting sexual or gender minorities are a “treatable disease.” These debates, naturally, often center on children.
Shrier believes that LGBQ youth are pressured into transitioning. She claims there are “many” desisters and detransitioners (citation?) and interviews a handful of them in her book. One regretted taking gender affirming hormones and having an orchiectomy; another subject “re-embraced her biological sex” and lesbian identity after identifying as trans from ages 13-19. Her story is certainly compelling, as she describes herself escaping the “grips of gender fever,” and identifies stress and academic pressure as the reasons for her trans identification. Another subject took testosterone in her 20s, at an age when she, according to Shrier, “no longer suffered from gender dysphoria” and realized that she would “never be fully accepted as a member of the transgender community without (testosterone).” This subject turned to the “gender critical” community of radical feminists and lesbians.
According to Shrier, the “circular logic that pervades trans ideology” states that “if you desist, you were never trans to begin with.” Shrier reports, “trans activists commonly deny there are any (detransitioners).” According to Shrier, detransition rates would be much higher, but “once you’ve been insisting to everyone that you’re one thing, it isn’t easy to announce (to everyone) that you might have made a mistake and change your mind.” Armed with a few anecdotal horror stories from detransitioners, Shrier attempts to establish as fact that detransition is common.
The first rigorous study on the factors that drive trans people to detransition was published this year. The study found that 13.1% of currently identified trans people had detransitioned at some point in their lives. 82.5% of them cited external factors, most commonly family pressure (35.5%), community pressure (32.5%), or trouble finding a job (26.8%). Other factors reported were non-affirming school and work environments, and an increased vulnerability to violence, including sexual assault. Detransition, transition regret, and surgical regret are three distinct phenomena frequently conflated by the media. Whether intentionally or not, data is used incorrectly, leading to alarming misinformation.
Detransition is a multifactorial phenomenon. There are trans people forced to (often temporarily) detransition due to barriers to living safely in their gender identity or expression, such as stigma, discrimination, and lack of access to care. Some trans people stop taking gender affirming hormones, for a multitude of reasons. Others report disappearance of gender dysphoria or distress. Many trans people do not desire medical intervention. Prior studies have included all of these situations in detransition statistics.
Detransition, even when it reflects a change in gender identity, often does not indicate regret. The media and certain experts understand detransition exclusively to mean transition regret.
Transition regret attributed to doubt about gender identity is expressed by 0.09% of people in one study, 0.3% in another, a rate of less than 1% in a third, and 2.4% in a fourth.
The medical research on gender affirming care yields very low rates of regret. Official statistics are difficult to obtain, however.
Surgical regret is related to disappointment with outcomes of gender affirming surgery rather than to a change in gender identity. The prevalence of regret after gender-affirmation surgery is extremely low, at < 1%. A retrospective study including 2,361 AFAB patients seen between 1972 and 2015 at the largest Dutch gender identity clinic which treats over 95% of the trans population in Netherlands, noted a regret rate of 0.3% for transmasculine people who underwent gonadectomy. Additionally, to allay Shrier’s fears, transmasculine people have been found to have more favorable psychosocial outcomes following surgery and are less likely to report post-surgical regret, despite a high rate of complications after gender affirming phalloplasty.
For reference, studies note that 28% of US AFAB people who had tubal sterilization reported regret. 23% of AMAB people who got treated for metastatic prostate cancer expressed regret. AFAB people who pursued excisional surgery for endometriosis or chronic pelvic pain reported a level of regret in 16.3% of patients. The surgical regret rate for gender affirmation surgery is one of the lowest.
A 2021 systematic literature review notes a dearth of research on desistance, and major methodological flaws in prior research studies. Factors such as an increase in trans visibility, acceptance and awareness, surgeon competency, cost of surgery, availability of surgery, insurance coverage, age, and race, also influence utilization of gender affirming surgeries. Future research might move away from attempting to predict gender identity outcomes and focus instead on reducing gender dysphoria distress in trans children.
Shrier’s alarm is nothing new; according to Christine Burns, British political activist and internationally recognized health adviser, fears around detransition have been used to delegitimize trans people for 40 years. Claims are always backed by anecdotal evidence as opposed to peer-reviewed research and weaponized by journalists to roll back legal progress.
Closing out the chapter, Shrier reassures us that there is “life after detransition.” After all, gender affirmation is a “travel toward (an) impossible horizon.”
Shrier’s solutions to the “transgender craze” oppose the gender affirmative approach: don’t affirm your child’s gender identity, push back, set limits, otherwise your child will “kick things up a notch.” Don’t expose your child to gender ideology by not allowing them to have a cell phone and making sure their school is not teaching LGBTQ history or anything but heteronormative sex ed. No discussion of sexual and gender minorities should be allowed, anywhere, anytime around your child. If your child is exposed to social media, make sure they don’t “come out” to strangers on the internet – it will be hard to take back later. If all else fails, move. Take your child out of college. Forbid them access to online LGBTQ communities. Find somewhere conservative values are enforced; your child will desist.
Conclusion: Somehow equality is still a topic of debate
Shrier sees gender affirmation as a constant uphill battle. ‘After all, you can only insist that you’re “trans” for so long before so many doubtful looks from peers silently prod: prove it.’
What an incredible mischaracterization of the trans community, and an unnecessary way to try to divide the trans community into “real” trans people and “fake” trans people! There is no “right” way to be trans. Trans people choose their own path of affirmation. There are those who affirm themselves socially, and those who do not. Those who affirm themselves medically, and those who do not, for a myriad of reasons. There are those who affirm themselves surgically, and those who do not. Additionally, social, medical, and surgical affirmation looks different for everyone. This does not make one person more valid than another. Trans people do not need to “prove” anything to anybody.
In April 2021, the American Medical Association urged legislators to oppose state laws that would prohibit medically necessary gender affirmation-related care for minor patients, and clearly stated that forgoing gender affirming care can have tragic mental and physical health consequences. As Physician Dr. Turban and Medical Historian Jules Gill-Peterson note, attacks on trans people are also attacks on science itself.
There are significant knowledge gaps in academic research on transgender health, especially in the fields of surgery, mental health, and endocrinology. Cisgender professionals have long dominated the field of trans healthcare, deciding what is important to research and writing about trans experiences from their perspective, a perspective that frames cis identities as “normal.” Advances in improving medical care for the trans community are tirelessly countered by stigma and discrimination; one small step forward means ten steps back. Epidemiologic studies suffer from selection bias. Mental health professionals evaluating trans patients for consideration of medical and surgical affirmation practice a heteronormative paternalism that places the burden on trans people to present “trans enough” to be deserving of care. Many factors make trans demographics difficult to study. Identifying people as trans may ‘out’ them when they are not out for their own safety. Most of the largest studies are anonymous online surveys. Electronic health records often do not record gender identity or sexual orientation data. Medical coding (ICD-11, CPT) falls short in identifying the entire range of gender affirming procedures. Patients are enrolled with insurance providers based on their legal gender marker, regardless of gender identity. A wide range of research methods confounds year-to-year comparison of prevalence. We need objective, accurate, and inclusive studies.
The trans community today, despite Shrier’s decrying of trans visibility as a “craze,” “agenda”, and “ideology,” faces an extreme amount of violence and opposition. Trans advocates speaking out for those stigmatized, marginalized, and ignored are often accused of silencing those who “oppose trans ideology.” Trans people are not a threat to free speech; instead, transphobic ideas often inform decisions around basic rights.
Congresswoman Marjorie Taylor Green has characterized The Equality Act, a landmark LGBTQ civil rights bill, as “disgusting, immoral, and evil.”
The opposition to The Equality Act is loud. In March, Shrier testified in the Senate against the Equality Act, on the basis that its protections for trans people would harm women and girls. She continues to assert her beliefs that trans women are not truly women, and that cis women are weak and must be protected from the transgender threat.
If passed, the bill would prohibit discrimination on the basis of sex, sexual orientation and gender identity in employment, housing, public accommodations, education, federally funded programs, credit, and jury service, and expand existing civil rights protections for people of color by prohibiting discrimination in more public accommodations, such as exhibitions, goods and services, and transportation.
Trans people are asking for basic legal protections across the country. Yet, somehow, in 2021, equality for all remains a hotly debated issue. The only trans agenda we have is living our lives.
Appendix
Editor’s note: Dr. Eckert’s Appendix to this reviews provides relevant background information that doesn’t really fit within the post but, I hope, will be useful and informative to our readers.
Abigail Shrier’s “Experts”
I will include here the experts Shrier thanks in her book: “Drs. Kenneth Zucker, Lisa Littman, Ray Blanchard, Paul McHugh, Will Malone, Michael Laidlaw, Patrick Lappert, J. Michael Bailey, Paul Hruz, and also Lisa Marchiano patiently improved my negligible understanding of gender dysphoria, human psychology, anatomy, and endocrinology.”
I am also including Sasha Ayad; though she does not appear in the above category, she is interviewed and cited quite frequently in Shrier’s book (Ayad, Sasha,6–7, 22, 154, 211, 213). Lisa Littman, another common source, is discussed ad nauseum in Part One. Though Shrier does interview Drs. Judy Chiasson, Hugh McLean and Randi Kaufman, and discusses Dr. Johanna Olson-Kennedy, their opinions are incongruent with Shrier et al’s ideas, and are not sourced, cited, or supported.
No beliefs are challenged in an echo chamber.
- Kenneth Zucker, PhD, Former Psychologist-in-Chief at Toronto’s Clarke Institute (now CAMH, the Adult Gender Identity Clinic of Toronto’s Centre for Addiction and Mental Health) and head of its Gender Identity Service from 2001-2014. Served on workgroups for DSM-IV, DSM-IV-TR, and chair of workgroup on “Sexual and Gender Identity Disorders” for DSM-5. Fired by CAMH in 2015, after Toronto introduced legislation banning conversion therapy. External review noted clinic to be an insular entity with an approach different from other gender clinics and out of step with current best practices. Decision supported by 1373 experts from several fields who work with trans kids.“The following recommendations are made to address clinical challenges identified: The current assessment and treatment approaches need to be revised. Gender variance versus gender dysphoria should be distinguished and explained. The aim to reduce suffering can be achieved with a client-centered and family supportive approach. To move towards this goal, it is recommended that WPATH, CPATH & AACAP guideline-informed care paths be utilized, across the age spectrum…”
- Ray Blanchard, PhD, Psychologist, Head of Clarke Institute 1980-1995, Head of CAMH’s Clinical Sexology Services from 1995–2010. Served on workgroups for DSM-IV Subcommittee on Gender Identity Disorders, DSM-5 committee. Resigned from HBIGDA (Harry Benjamin International Gender Dysphoria Association, now WPATH) in 2003.
- Paul McHugh, MD, University Distinguished Service Professor of Psychiatry, Director of the Department of Psychiatry and Behavioral Science at Johns Hopkins 1975-2011. Shut down gender clinic at Johns Hopkins in 1979, citing “no change in psychological condition” of trans people post-gender affirming surgery. Served on the Roman Catholic Church’s national sexual abuse review board testifying on behalf of people accused of child abuse.
- Will Malone, MD, Internist, subspecialty certification in Endrocrinology
- Michael Laidlaw, MD, Endocrinologist
- Patrick Lappert, MD, Plastic Surgeon, Catholic Deacon in Alabama
- J. Michael Bailey, PhD, Professor of Psychology at Northwestern University. Wrote The Man Who Would Be Queen in 2003. In 2004 Bailey was accused of providing clinical psychology services without a license in the form of letters of support for patients for sex reassignment surgery (SRS). (These claims were apparently not pursued by the State of Illinois because Bailey did not charge for these services and therefore his actions were not illegal in the State of Illinois.) [The previous passage has undergone clarification. See Addendum for explanation.] In 2011, Northwestern stopped Bailey’s Human Sexuality course: “On Monday more than 100 students watched the optional after-class demonstration, during which a woman got undressed, lay down on a towel and allowed her fiance to penetrate her with a device that looks like a machine-powered saw with a phallic object instead of a blade. The demonstration followed a discussion about kinky sex and female orgasm.”
- Paul Hruz, MD, PhD, Pediatrician and Pediatric Endocrinologist, Associate Professor of Pediatrics, Washington University in St. Louis. According to Washington University, has not treated any trans patients.
- Lisa Marchiano, LCSW, “Jungian Analyst“
- Sasha Ayad, LPC, “works in private practice with teens and young adults who are questioning their gender.”
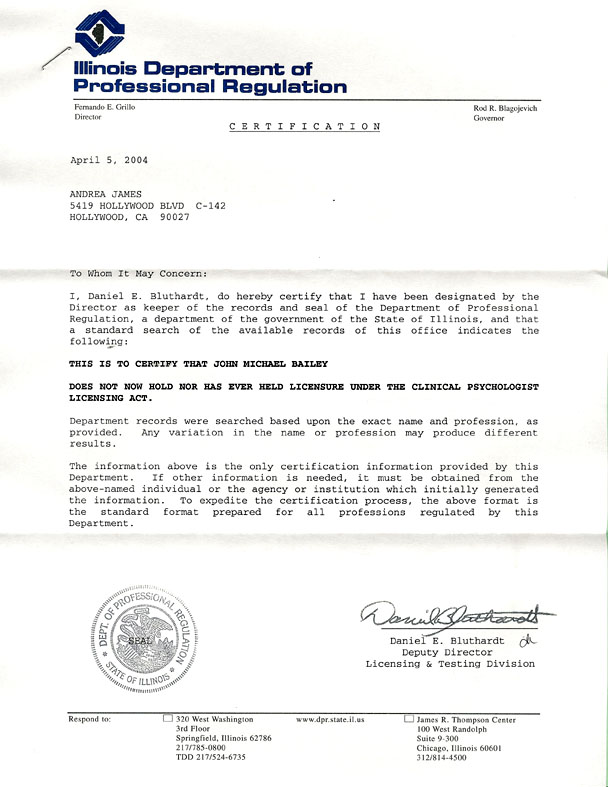{kind=link}
Affiliations
American College of Pediatricians (ACP): not to be confused with the American Academy of Pediatricians (AAP). AAP, founded in 1930, supports gender affirmative care. “We’re 67,000 pediatricians committed to the optimal physical, mental, and social health and well-being for all infants, children, adolescents, and young adults.” ACP is designated an extremist hate group by the Southern Poverty Law Center. Socially conservative advocacy group founded in 2002, as a protest against AAP’s support for adoption by gay couples. 200-500 members. Works closely with NARTH.
- McHugh, member. 2016/2017: Gender Ideology Harms Children
- McHugh/Laidlaw/Hruz/Bailey cowriters, 12/4/2018: ACP Letter to USDoJ, USDHHS, US Dept of Education
- Laidlaw/Hruz/Malone 2019 Letter to the Editor: “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline”
GD (Pediatric and Adolescent Gender Dysphoria) Working Group: not to be confused with the GDA (Gender Dysphoria Affirmative) Working Group. GDA Working Group is “a group of medical and mental health professionals, academics, researchers, activists, and allies, some trans and others cis, devoted to the health and happiness of transgender and gender nonconforming youth. Most of us have extensive experience working directly with trans youth.” GD Working Group is “an international group of psychiatrists, psychologists, clinical social workers, researchers, and psychoanalysts that have a special interest in the treatment of GD in children, adolescents, and young people. Many of us have come to be concerned about the sharply rising numbers of young people presenting with gender dysphoria, and the current trend to affirm them and in many cases move toward social and medical intervention. We wish to discuss the evidence for this rise in trans identified referrals and explore the evidence that social contagion may be at play, particular for those young people presenting with rapid onset gender dysphoria (ROGD) in adolescence.”
- Zucker, member
- Blanchard, member
- Bailey, member
- Malone, member, Gender Dysphoria Resource for Providers cites Blanchard, Bailey, Zucker, Littman, Shrier, McHugh
- Ayad, member
- Laidlaw, member, columnist The Gender Identity Phantom
- Marchiano, member
Alliance Defending Freedom (ADF): designated as an extremist hate group by the Southern Poverty Law Center
- McHugh/Hruz
- 2016: Amicus briefs filed with Supreme Court in Gloucester County-case of transgender student denied use of men’s room at his Virginia high school
- 2018: Amicus briefs filed with Appellate Court in Palatine, Illinois-case of transgender student denied use of girl’s locker room at her Illinois high school
- Hruz: 2017 Amicus brief filed with US District Court in Jacksonville, Florida-case of transgender high school student denied access to boys’ restroom
The New Atlantis Journal of Technology & Society: a non-peer-reviewed medical journal. “We are not an academic journal but a public journal of ideas.” Published by the Ethics and Public Policy Center (EPPC), a Christian conservative think tank that supported Defense of Marriage Act, Don’t Ask, Don’t Tell, and is in favor of religious freedom acts.
- McHugh Fall 2016: The New Atlantis Special Report Sexuality and Gender
- Hruz/McHugh cowriters 2017: Growing Pains: Problems with Puberty Suppression in Treating Gender Dysphoria
Archives of Sexual Behavior, The Official Publication of the International Academy of Sex Research.
- Zucker, Editor-in-Chief, 2001 – current
- Founding Editor 1971-2001 Richard Green, MD, JD specialized in GID. Collaborated with John Money, Harry Benjamin. Founding committee member of HBIGDA, President 1997-1999. Coined “gender identity disorder.” Argued in favor of declassification of homosexuality. Served on DSM-IV committee. The “Sissy Boy Syndrome” and the Development of Homosexuality (Green 1987) study of 66 gender-atypical boys who stated they wished to be girls noted that 75% of these boys grew up to be gay men.
- Blanchard, Editorial Board
- Bailey, Editorial Board
- Littman, Editorial Board
- Blanchard, columnist
- Bailey, columnist
- Malone, columnist
- Ayad, columnist, listed under therapy resources
- Marchiano, columnist
Society for Evidence-Based Gender medicine, founded 2020. “An international group of over 100 clinicians and researchers concerned about the lack of quality evidence for the use of hormonal and surgical interventions as first-line treatment for young people with gender dysphoria. We represent expertise from a range of clinical disciplines. Our objectives include evaluating current interventions for gender dysphoria, providing balanced evidence summaries, promoting the development of effective and supportive psychosocial approaches for the care of young people with gender dysphoria and generating good, answerable questions for research.”
- Malone, Board of Directors
- Marchiano, member
- Ayad, member
The Heritage Foundation, American conservative think tank, runs a blog The Daily Signal
- Laidlaw 2019 panelist “The Medical Harms of Hormonal and Surgical Interventions for Gender Dysphoric Children,” on YouTube.
- Hruz 2017 panelist “Gender Dysphoria in Children: Understanding the Science and Medicine,” on YouTube.
Focus on the Family, an American fundamentalist Christian organization
- Laidlaw: 2020 testified before South Dakota House State Affairs Committee in support of South Dakota HB 1057-bill that prohibits medical professionals from performing “sex change” procedures on minors “Vulnerable Child Protection Act.” HB 1057 also prohibits medical professionals from giving medication such as puberty blockers or “cross-sex” hormones to minors for the same reason.
ReIMe (Rethink Identity Medicine Ethics): “devoted to questioning the gender affirmative model and exploring alternatives for gender variant children and adolescents.” Position Statement
- Marchiano, Board of Directors
- Malone, Advisory Board
- Resources: Shrier book, articles by Littman, Marchiano
- Links to websites: SEGM, gdworkinggroup.org
Alliance for Therapeutic Choice and Scientific Integrity: formerly NARTH (National Association for Research and Therapy of Homosexuality) “A multi-disciplinary professional and scientific organization dedicated to preserving the right of individuals to obtain the services of a therapist who honors their values, advocating for integrity and objectivity in social science research, and ensuring that competent licensed, professional assistance is available for persons who experience unwanted homosexual attractions.”
- “The Alliance for Therapeutic Choice and Scientific Integrity believes that there there are significant psychological, medical and societal risks associated with attempts to alter someone’s biological sex through hormone therapy or sexual reassignment surgery.”
- Associated with American College of Pediatricians (Executive Director of ACP is on Medical Division Committee of Alliance), sources work by Marchiano, McHugh, Laidlaw, Zucker, Littman, Bailey
June 10, 2021 HANDOUT Health and Human Services Interim Committee, Utah State Legislature. TRANSGENDER “TRANSITION” PROCEDURES PERFORMED ON MINORS ANSWERS TO QUESTIONS AND INFORMATION FOR JOINT INTERIM COMMITTEE
- Hruz/Lappert/Laidlaw/McHugh cowriters: “…clearly children and adolescents cannot provide informed consent. The version of the suggested legislation considered in the general session earlier this year would not have criminalized performing attempted sex-change surgery on a minor female (assuming the parents consented), but would have defined performing such procedures on a minor as unprofessional conduct that could lead to revoking the medical license of the surgeon performing the procedure. If a measure such as the suggested legislation is enacted, the exemption from criminal prosecution in section 76-5-702(3) could remain unchanged. However, to avoid ambiguity, the legislation should provide specifically for the possibility of professional discipline notwithstanding the exemption from criminal sanction. It should also provide that the private right of action in section 76-5-704 applies and that parental consent is not a defense to a private right of action.”
Claim: Trans Children = Homosexual Adults
- Blanchard/Bailey: 2017 Gender dysphoria is not one thing blog post on 4thWaveNow
- “The first type–childhood-onset gender dysphoria—definitely occurs in both biological boys and girls. It is highly correlated with homosexuality–the sexual preference for one’s own biological sex–especially in natal males.”
- Malone: 2019 No Child is Born in the Wrong Body … and other thoughts on the concept of gender identity
- “However, starting at a young age, children do tend to exhibit preferences and behaviors that we associate with sex. For example, male children display more aggressive behavior than female children. In addition, “cross-sex” behavior, or more accurately cross-sex stereotypical behavior, is often predictive of later same-sex attraction.”
- Ayad: 2019 The Same but Different: Convergent Pathways of Gender Dysphoria
- “It’s also likely that engagement in a community of women with similar experiences mightalleviate her dysphoria without requiring medical intervention. Cindy may ultimately embrace her sexuality and perhaps identify as a “butch” lesbian.”
- 2021 A Counselor Explains How Conversion Therapy Bans Can Cause Harm: “…many of my female clients began noticing their romantic attractions towards other girls in the pre-teen years. Despite having open-minded attitudes towards homosexuality, they felt confused and ambivalent about their emergent sexuality. In these cases, searching online for explanations of their same-sex attraction lead them consider if they may have a “male gender identity.”
- Marchiano: 2017 “Outbreak: On Transgender Teens and Psychic Epidemics” (Psychological Perspectives)
- “Most of those who desist will come out to be lesbian or gay.”
- “Lesbians are particularly worried about the teen trans trend, as most girls coming out as transgender are same-sex attracted (Kreher,2016). Many in the lesbian community are distraught to notice that butch lesbians are quickly disappearing“
- Zucker/Blanchard cowriters, 2017 The Prevalence of Only-Child Status Among Children and Adolescents Referred to a Gender Identity Service Versus a Clinical Comparison Group
- “Reason for referral to the gender identity service included persistent cross-gender behavior and/or identification, transvestic fetishism (sensu DSM-III and DSM-IV-TR; American Psychiatric Association, 1980, 2000), or reasons related to homosexual sexual orientation. Gender-referred children aged 12 or younger were classified as homosexual in relation to natal sex, because follow-up studies have demonstrated that this is the most probable outcome for this population (Green, 1987; Singh, 2012; Steensma, 2013; Wallien & Cohen-Kettenis, 2008).
- Children referred for transvestic fetishism were categorized as (pre)heterosexual, as it is characterized by attraction to females (Zucker & Blanchard, 1997). Gender-referred adolescents were categorized as heterosexual or homosexual based on clinical diagnostic information or the Erotic Response and Orientation Scale (Storms, 1980) and the Sexual History Questionnaire (Langevin, 2013).”
Claim: Gender Affirmation Doesn’t Work
- McHugh Fall 2016: The New Atlantis Special Report Sexuality and Gender
- “Compared to the general population, adults who have undergone sex reassignment surgery continue to have a higher risk of experiencing poor mental health outcomes. One study found that, compared to controls, sex-reassigned individuals were about five times more likely to attempt suicide and about 19 times more likely to die by suicide.”
- Blanchard/Bailey: 2017 Suicide or transition: The only options for gender dysphoric kids? Blog post on 4thWaveNow
- “We have already mentioned the fact that transitioned adults who had been gender dysphoric (i.e., “transsexuals”) have increased rates of completed suicide. Their transition did not prevent this, evidently.”
- Laidlaw/Hruz/Malone Letter to the Editor: “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Practice Guideline”
- “Furthermore, limited long-term outcome data fail to demonstrate long- term success in suicide prevention”
- Lappert Sep 2019: Plastic surgeon: Sex-change operation ‘utterly unacceptable’ and a form of ‘child abuse’ on Blog Truth is the New Hate Speech
- “After a period of observation beyond some eight to 10 years, the suicide rate goes right back to where it was if nothing had been done for these people. If you didn’t offer them any care at all, you’d have the same suicide rate that people have now after all of the surgical interventions,” said Lappert. “And after the excitement dies down, and eight, 10 years later, they’re right back to a 40 to 42 percent suicide rate. So that’s a huge misrepresentation of benefit that is just not true.”
- Ayad 2020: Parallels Between Lobotomy and Childhood “Gender” Transition
- “Serious examination of the current data shows little scientific value for either lobotomy or youth medical transition”
- McHugh/Laidlaw/Hruz cowriters, 12/4/2018: ACP Letter to USDoJ, USDHHS, US Dept of Education
- “Social and medical “gender transition and affirmation,” however, is not proven to decrease suicide rates.”
- Marchiano 2020: The Ranks of Gender Detransitioners are Growing. We Need to Understand Why
- “For most of these young women, identifying as trans worsened their mental health. Although some report that starting on hormones initially brought an increase in confidence and well-being, these drugs eventually seemed to make some of them more emotionally labile, and intensified depression and suicidality. Some of the women who underwent surgeries such as mastectomies or hysterectomies found that these procedures brought no relief from their suffering and instead resulted in nerve damage, regret and, in some cases, life-long dependence on synthetic hormones.”
Appeal to Biology
- McHugh Fall 2016: The New Atlantis Special Report Sexuality and Gender
- “In reviewing the scientific literature, we find that almost nothing is well understood when we seek biological explanations for what causes some individuals to state that their gender does not match their biological sex…”
- Blanchard: 2019 Twitter thread
- “The sex of a postoperative transsexual should be analogous to a legal fiction. This legal fiction would apply to some things (e.g., sex designation on a driver’s license) but not to others (entering a sports competition as one’s adopted sex).”
- Laidlaw: 2019, YouTube video. Medical Risks of Hormonal and Surgical Interventions for Gender Dysphoric Children
- “There are only two sexes. Certain science publications want you to think there’s more and to think it’s a spectrum. Sex is identified at birth, nobody assigns it…we all know how to identify it.”
- Malone: 2019 No Child is Born in the Wrong Body … and other thoughts on the concept of gender identity
- “Our culture-at-large is incorrectly telling them that they may have been born in the wrong body. The propagation of this biological falsehood, in addition to other newly identified factors, is likely contributing to the growing number of transgender identifying high school students (now estimated to be 2%), and the rapid rise in adolescents presenting to gender clinics.”
- 2019 Gender Dysphoria Resource for Providers
- “Medically, the term transgender/transsexual refers to an individual who has taken significant steps to present themselves to society as the opposite sex, in an effort to relieve severe and persistent gender dysphoria. No one is born transgender or transsexual and no serious scientist has ever made such a claim. It is not possible to be born into the “wrong” body (“boy brain” in a girl body for example).”
- Lappert Sep 2019: Plastic surgeon: Sex-change operation ‘utterly unacceptable’ and a form of ‘child abuse’
- Asked “What is a sex change?” Lappert responded, “Well, to begin with, the idea that you can change someone’s sex is a lie.”
- “Many people have been led to believe by a lot of very clever programs and advertising from plastic surgeons and whatnot that you can actually change a man into a woman or a girl into a boy or anything like that,” he said. “You cannot. Essentially all you can do is you can modify people’s bodies both with medicines as well as with surgery to make them appear to be the other sex, but they will never be the other sex.”
- Marchiano: 2017 “Outbreak: On Transgender Teens and Psychic Epidemics” (Psychological Perspectives)
- “However, to date, the notion of an innate gender identity is not supported by science.”
- McHugh/Laidlaw/Hruz cowriters, 12/4/2018: ACP Letter to USDoJ, USDHHS, US Dept of Education
- “Applaud Trump Administration’s attempt to uphold the scientific definition of sex in federal law and policy…Human sex is a binary, biologically determined, and immutable trait from conception forward…Gender identity is not an immutable trait…Individuals who identify as transgender may have mistaken beliefs about themselves and their bodies.”
Claim: Very High “Desistance” Rates
- Zucker The myth of persistence: Response to “A Critical Commentary on Follow-Up Studies and “Desistance” Theories about Transgender and Gender Non-Conforming Children” by Temple Newhook et al. (2018). International Journal of Transgenderism.
- 2018. The Myth of the “Desistance Myth”
- “I would hypothesize that when more follow-up data of children who socially transition prior to puberty become available, the persistence rate will be extremely high. This is not a value judgment—it is simply an empirical prediction . . . parents who support, implement, or encourage a gender social transition (and clinicians who recommend one) are implementing a psychosocial treatment that will increase the odds of long-term persistence.”
- 2018. The Myth of the “Desistance Myth”
- Laidlaw/Hruz/Malone Letter to the Editor: “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Practice Guideline”
- “Children with GD will outgrow this condition in 61% to 98% of cases by adulthood.”
- Hruz/McHugh cowriters 2017. Growing Pains: Problems with Puberty Suppression in Treating Gender Dysphoria
- “Most children with gender identity problems eventually come to accept the gender associated with their sex and stop identifying as the opposite sex.”
- Marchiano: 2017 “Outbreak: On Transgender Teens and Psychic Epidemics” (Psychological Perspectives)
- “There is a wealth of replicated research that tells us that 80–95% of children who experience a cross-sex identification in childhood will eventually desist and come to identify with their natal sex as adults.”
- Lappert Sep 2019. Plastic surgeon: Sex-change operation ‘utterly unacceptable’ and a form of ‘child abuse’
- Lappert also warned that a whole generation of children is being raised whose psychosexual, physical, and neurological development are being stunted in hopes of supporting this cross-sex idea of themselves – pushed by the transgender industry. He pointed out that if you took 100 children with cross-sex idea of themselves, 91 percent of them will desist. “Ninety-one percent of them will stop thinking of themselves as the other sex,” said Lappert. “But if you take the same hundred children to a transgender clinic at your local urban center, 100 percent of them will persist in it, which on the face of it tells you that this is this is the malpractice of medicine…If 91 percent of them would have gotten over the disease and 100 percent of them persistent and obviously you’re doing something wrong here,” he added. “But nonetheless that’s how it’s being presented.”
- Bailey 2015: Op-Ed: What should you do if your son says he’s a girl?
- “Gender dysphoric children have not usually become transgender adults. For example, the large majority of gender dysphoric boys studied so far have become young men content to remain male. More than 80% adjusted by adolescence.”
Don’t Call it Conversion Therapy
(For an overview on conversion therapy, see It’s Torture not Therapy).
- Zucker 12/1/2020. House of Commons Standing Committee of Justice and Human Rights, Bill C-6 An Act to amend the Criminal Code (conversion therapy)
- “In my view, Bill C-6 should be modified in one of two ways. One is to delete entirely any reference to gender identity and restrict it to sexual orientation, the original target of criticism of conversion therapy. Failing that, Bill C-6 should be extensively revised in terms of explaining the scope of what exactly it means to engage in exploration of gender identity or its development—in other words, provide objective markers. Such a revision would help both clinicians and families that have a child or adolescent experiencing gender dysphoria understand what the legislation truly intends to target.”
- Zucker: 2018 article Zucker Defied Trans Orthodoxy. Now He’s Vindicated.
- “Though he will sometimes recommend social and medical transition for his patients, Dr. Zucker is guided by the general principle that congruence between a patient’s gender identity and birth sex is the ideal outcome. This approach is informed by decades of case-by-case clinical practice and a small but substantial body of research — in an uncertain and under-researched area — suggesting that over two-thirds of children with gender dysphoria will realign with their birth sex by the end of adolescence if they have not been exposed to transition-based treatments.”
- 2008 Task Force questions critical appointments to APA’s Committee on Sexual and Gender Identity Disorders
- “WASHINGTON, May 28 —The National Gay and Lesbian Task Force is questioning the American Psychiatric Association’s (APA) recent appointments of Kenneth Zucker, Ph.D., to chair the Committee on Sexual and Gender Identity Disorders for the revision of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), and Ray Blanchard, Ph.D., to serve as a committee member. These appointments are raising great concerns within the lesbian, gay, bisexual and transgender community. Zucker has built his reputation on the position that children can be directed away from nonconforming gender expression via therapy, while Blanchard has a long list of articles pathologizing commonplace expressions of sexuality and gender. In 1973, the Task Force was instrumental in getting the APA to declassify homosexuality as a mental disorder.
- “We are very concerned about these appointments. Kenneth Zucker and Ray Blanchard are clearly out of step with the occurring shift in how doctors and other health professionals think about transgender people and gender variance. It is extremely disappointing and disturbing that the APA appears to be failing in keeping up with the times when it comes to serving the needs of transgender adults and gender-variant children.”
- July 2020 Twitter thread on Dr. Robert Spitzer reporting that Spitzer regretted the study that he did “because it would taint his legacy.”
- Background: Robert Spitzer (1932-2015): 1973-led effort to stop treating homosexuality as mental illness; 1974-Chair of APA’s task force on DSM-III; 2001 paper- “Can Some Gay Men and Lesbians Change Their Sexual Orientation?” argued that highly motivated people could become heterosexual. Article played a huge role in encouraging and allowing conversion therapy.
- 2001-APA issued official disavowal of paper-no peer review, no published scientific evidence to support
- 2003-paper published in Archives of Sexual Behavior (Editor Zucker)
- 2012-Spitzer repudiated and apologized for 2003 publication on reparative therapy
- McHugh 2017: Human Rights Campaign Response to Amicus Brief of Paul R. McHugh, M.D., et al. in Support of Defendant-Appellee
- “Paul McHugh, a psychiatrist at Johns Hopkins University, has repeatedly filed amicus briefs in cases concerning the civil rights of lesbian, gay, bisexual, transgender and queer (LGBTQ) people. His investment in these cases is puzzling, because McHugh’s research career has never touched on gender identity or sexual orientation, nor does he appear to have clinical experience with LGBTQ patients. Nonetheless, in early 2017, McHugh filed a brief in the Supreme Court of the United States arguing against transgender student Gavin Grimm’s right to use gender-appropriate restrooms in his Gloucester, VA high school. Listed as coauthors were diabetes researcher Paul Hruz and biostatistician Lawrence Mayer; like McHugh, neither coauthor appears to have clinical or research experience with transgender children or adults. This lack of expertise may explain why the brief itself is filled with misunderstandings and misstatements about transgender children and teens. Below, we address three primary areas of inaccuracy: unsubstantiated and widely rejected claims about “conversion therapy”; misinformation about gender-affirming care; and crucial school climate research that the brief fails to address. The most concerning section of the brief is the assertion that conversion therapy—that is, a range of practices intended to change a person’s sexual orientation or gender identity—is an appropriate response to transgender youth.”
- Blanchard/Bailey: 2017 Gender dysphoria is not one thing blog post on 4thWaveNow
- “If you want your childhood-onset gender dysphoric child to desist, and if your child is still well below the age of puberty (which varies, but let’s say, younger than 11 years), you should firmly (but kindly and patiently) insist that your child is a member of his/her birth sex. You should consider finding a therapist if this is difficult for you and your child. You should not allow your child to engage in behaviors such as cross dressing and fantasy play as the other sex. Above all else, you should not let your child socially transition to the other sex.”
- Ayad: 2019 The Same but Different: Convergent Pathways of Gender Dysphoria
- “Embodiment exercises could help her relate more gently to her body. And with the therapist modeling curiosity and support, she might explore what masculinity means to her”
- 2021 A Counselor Explains How Conversion Therapy Bans Can Cause Harm
- “If conversion therapy bans include gender identity, therapy will either affirm same-sex attraction or it will affirm gender identity. We can’t simultaneously affirm both, since biological sex is the basis of sexual orientation.”
- 2019 YouTube video Identity, Gender, Adolescence, & Therapy with Sasha Ayad
- “A therapist would feel obliged to agree emphatically with a client’s gender self-concept. In the above examples, had therapy prioritized gender affirmation, these young women might now be in the process of making unnecessary and irreversible medical changes to their healthy bodies in an attempt to become boys.”
- Marchiano/Ayad cowriters with members of SEGM, 2021 “One Size Does Not Fit All: In Support of Psychotherapy for Gender Dysphoria.” Archives of Sexual Behavior50/1 (2021), 7-16.
- A critique of Turban, Beckwith, Reisner, and Keuroghlian’s (2020) article that equates all non-Gender Affirming therapeutic approaches to GD as “conversion therapy” that leads to poor mental health/suicidality.
- Laidlaw 2018: The Gender Identity Phantom
- “This condition comes down to a mental state of being. In other words this feeling that a girl with a girl’s body is inside a boy is simply that, a feeling. No matter how deeply or strongly this is felt, the material reality is that this person is a girl.In the past psychologists and psychiatrists such as Ken Zucker and Susan Bradley had been able to work with children and adolescents whose internal feeling of being a boy for example did not match their physical sex. There was success in using psychological methods to resolve this conflict. Currently, licensed therapists such as Sasha Ayad carry on similar work successfully. This type of care has been completely excluded as a possibility in the AAP’s narrow treatment design, as has watchful waiting.”
- Hruz 2019: Deficiencies in Scientific Evidence for Medical Management of Gender Dysphoria
- “The pioneering work of Zucker established that many but not all patients who received psychological counseling and support were able to manage and resolve conflicts arising from discordant gender identity, particularly in affected children (Zucker et al. 2012).”
Claim: Children Too Young to Know if They’re Trans
- Zucker: 2017 BBC Documentary “Transgender Children: Who Knows Best?”
- “a four-year-old might say that he’s a dog – do you go out and buy dog food?”
- Hruz/McHugh cowriters 2017: Growing Pains: Problems with Puberty Suppression in Treating Gender Dysphoria
- “Moreover, children are not fully capable of understanding what it means to be a man or a woman.
- Lappert Sep 2019: Plastic surgeon: Sex-change operation ‘utterly unacceptable’ and a form of ‘child abuse’
- “Children do not have the capacity to consent to those sorts of treatments,” Lappert said of sex-change procedures. “You cannot tell a pre-adolescent child anything about their adult life and expect that they’re going to understand what you’re telling them.”
- “Their concept of themselves is in the formative years,” he continued. “And to ask a child to think of their sexuality when they’re pre-adolescent is utterly insane. And it’s in fact another great evil that’s being inflicted upon children because it’s the sexualization of normal chaste friendships of childhood.”
- Malone cowriter, 2019: No One is Born in ‘The Wrong Body’
- “Developmental studies show that young children have only a superficial understanding of sex and gender (at best). For instance, up until age 7, many children often believe that if a boy puts on a dress, he becomes a girl. This gives us reason to doubt whether a coherent concept of gender identity exists at all in young children. To such extent as any such identity may exist, the concept relies on stereotypes that encourage the conflation of gender with sex.”
Claim: Trans Youth Suicide Rates are Spurious
- Zucker: 2017 article Transgender Kids: why doctors are right to be cautious about childhood transition
- “Zucker points out that his research has found suicidality among trans children is no higher than among children with depression, anxiety or ADHD”
- 2019 presentation #GIDYVR: Gender Identity and Kids
- Blanchard/Bailey: 2017 Suicide or transition: The only options for gender dysphoric kids? Blog post on 4thWaveNow
- “Why would anyone falsely report being suicidal? One reason is to influence the behavior of others. Saying that one is suicidal usually gets attention–sympathy, for example. It can be a way of impressing others with the seriousness of one’s feelings or needs.”
- Marchiano: 2018Transgenderism and the Social Construction of Diagnosis
- “In addition, the widely cited suicide rate that is often mentioned as a justification for urgent intervention is based on a study which does not prove that there is a causal link between gender transitioning and improvement in mental health. It is still unknown whether transition changes suicide rates for gender dysphoric individuals.”
Claim: Rapid Onset Gender Dysphoria
- Zucker: 2018 Twitter: “Lisa Littman’s important paper on rapid-onset gender dysphoria is now online at PLoSONE. It is open access, so anyone can download the link.”
- Blanchard/Bailey: 2017 Gender dysphoria is not one thing blog post on 4thWaveNow
- The third type—rapid-onset gender dysphoria—mostly occurs in adolescent girls. This type is primarily characterized by the age and speed of onset rather than the associated sexual orientation, and it may not be limited to one sex, as the second type is. Our impression is that rapid-onset gender dysphoria is especially common among daughters of parents who read 4thWaveNow as well as those who post on the support board at gendercriticalresources.com.
- Laidlaw/Hruz/Malone Letter to the Editor: “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Practice Guideline”
- “The recent phenomenon of teenage girls suddenly developing GD (rapid onset GD) without prior history through social contagion is particularly concerning.”
- Laidlaw: 2019, YouTube video. Medical Risks of Hormonal and Surgical Interventions for Gender Dysphoric Children
- “there’s a newer phenomenon…of teenage girls developing this condition…binge-watching Youtube videos seems to be playing a role, social contagion seems to be playing a role.”
- Lappert: 2021 YouTube: “Puberty is NOT a disease”
- “A 2019 study showed that when a teen announces a transgender identity to their peer group, the number of friends who also became transgender was 3.5 per group”
- Marchiano: 2017 “Outbreak: On Transgender Teens and Psychic Epidemics” (Psychological Perspectives)
- “My fear—and I am hardly alone in this—is that adopting a transgender identity has become the newest way for teen girls to express feelings of discomfort with their bodies—an issue adolescent girls typically experience. The problem here is that many young women are seeking transition after coming to identify as transgender, and transition can have extreme consequences.”
- Ayad: 2019 The Same but Different: Convergent Pathways of Gender Dysphoria
- “Around 2013, however, something shifted dramatically. Gender clinics began documenting soaring numbers of teens, mostly girls, seeking help for gender-related distress.”
- McHugh 2019 Psychiatrist Compares Experiments on Children Claiming to Be Transgender to ‘Frontal Lobotomies’
- “McHugh observed this theory was suggested in a study conducted by Dr. Lisa Littman on rapid onset gender dysphoria (ROGD).”I believe that these gender confusions are mostly being driven by psychological and psychosocial problems these people have,” he said. “That explains the rapid onset gender dysphoria Lisa Littman has spelled out.””
- Malone/Laidlaw/Hruz 2019 Letter to the Editor: “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Practice Guideline”
- “There are no laboratory, imaging, or other objective tests to diagnose a “true transgender” child. Children with GD will outgrow this condition in 61% to 98% of cases by adulthood. There is currently no way to predict who will desist and who will remain dysphoric. The degree to which GAT has contributed to the rapidly increasing prevalence of GD in children is unknown. The recent phenomenon of teenage girls suddenly developing GD (rapid onset GD) without prior history through social contagion is particularly concerning.”
Claim: Social Affirmation Leads to Trans Identity Persistence
- Zucker 2018: The myth of persistence: Response to “A Critical Commentary on Follow-Up Studies and “Desistance” Theories about Transgender and Gender Non-Conforming Children” by Temple Newhook et al. (2018). International Journal of Transgenderism. https://doi.org/10.1080/15532739.2018.1468293
- “ I would argue that parents who support, implement, or encourage a gender social transition (and clinicians who recommend one) are implementing a psychosocial treatment that will increase the odds of long-term persistence.”
- 2019 “Debate: Different Strokes for Different Folks”
- “A gender social transition in prepubertal children is a form of psychosocial treatment that aims to reduce gender dysphoria, but with the likely consequence of subsequent (lifelong) biomedical treatments as well (gender‐affirming hormonal treatment and surgery).Gender social transition of prepubertal children will increase dramatically the rate of gender dysphoria persistence when compared to follow-up studies of children with gender dysphoria who did not receive this type of psychosocial intervention and, oddly enough, might be characterized as iatrogenic. Parents who bring their children for clinical care hold different philosophical views on what is the best way to help reduce the gender dysphoria, which require both respect and understanding.”
- Blanchard/Bailey: 2017 Gender dysphoria is not one thing blog post on 4thWaveNow
- A recent study found that social transition was the most powerful predictor of persistence among natal males. That is, gender dysphoric boys allowed to live as girls strongly tended to want to become adult women. (The same trend occurred for natal females, but it was less robust.) This is not surprising. If a gender dysphoric child is allowed to live as the other sex, what will change his/her mind? No one disputes that gender dysphoric children really, really would like to change sex.
- Malone: 2019 No Child is Born in the Wrong Body … and other thoughts on the concept of gender identity
- “a child that he or she was born in the wrong body pathologizes “gender non-conforming” behavior and makes gender dysphoria less likely to resolve”
- Hruz/McHugh cowriters 2017: Growing Pains: Problems with Puberty Suppression in Treating Gender Dysphoria
- “However, the medical treatments provided for children with apparent symptoms of gender dysphoria, including affirmation of gender expression…may drive some children to persist in identifying as transgender when they might otherwise have, as they grow older, found their gender to be aligned with their sex”
- Marchiano 2017: “Outbreak: On Transgender Teens and Psychic Epidemics” (Psychological Perspectives 2017)
Claim: Autogynephilia is Real
Blanchard coined the term autogynephilia to define the propensity of AMAB trans people to be sexually aroused by cross-gender ideation, leading to his taxonomy of transfeminine people:
This classification reduces trans people to sexual paraphilias.
“Homosexual transsexuals” (AMAB women attracted to men). This gets confusing since trans women attracted to only men would be heterosexual, but this is Blanchard’s classification and language.
- “homosexual transsexuals” don’t report sexual arousal from thoughts of being feminine
- Effeminate boys or masculine girls who would grow into gay men and women
“Heterosexual transsexuals” (AMAB women attracted to women)
- “less feminine in childhood”
- “request sex reassignment” at a later age
- “histories of erection during cross-dressing” (Blanchard 1985)
- more likely to report erotic arousal with thoughts of themselves as women (Blanchard 1989a)
- “I’ve published two studies that suggest at least some transsexuals who deny autogynephilic arousal are consciously or unconsciously distorting their histories. How does one decide when the discrepant self-reports of a minority of patients indicate psychological denial and when they indicate a bona fide separate syndrome?” (Blanchard 2003)
- Blanchard: originated the idea. 2008, Deconstructing the Feminine Essence Narrative: Blanchard’s commentary on Alice Dreger’s book which covering the controversy surrounding Bailey’s book on Blanchard’s autogynephilia theory
- Bailey: wrote a book about Blanchard’s theory. 2003, The Man Who Would Be Queen: The Science of Gender-Bending and Transsexualism
- McHugh: 2015 Transgenderism: A Pathogenic Meme
- “I have not met or examined Jenner, but (his) behavior resembles that of some of the transgender (males) we have studied over the years. These (men) wanted to display themselves in sexy ways, wearing provocative female garb. More often than not, while claiming to be a woman in a man’s body, they declared themselves to be “lesbians” (attracted to other women). The photograph of the posed, corseted, breast-boosted (Bruce) Jenner (a (man) in his mid-sixties, but flaunting (himself) as if a “pin-up” girl in her twenties or thirties) on the cover of Vanity Fair suggests that (he) may fit the behavioral mold that Ray Blanchard has dubbed an expression of “autogynephilia”—from gynephilia (attracted to women) and auto (in the form of oneself).”
- Malone 2019 Gender Dysphoria Resource for Providers
- “Etiology: Gender dysphoria always has an underlying cause. Those main causes include: 1) autogynephilia (a heterosexual male who is sexually aroused at the thought of himself as a woman), or 2) rejection of one’s homosexuality (for example preference to live life as a “trans woman”, attracted to men, vs a gay man), or 3) is the consequences of concrete thinking processes that characterize autism spectrum conditions (“I don’t like dresses therefore I must be a boy”), or 4) is a protective mechanism to avoid repeat sexual trauma, or 5) is due to the stress of simply not fitting into society’s stereotypical expectations of gender roles. No one is born in the wrong body. That’s biologically impossible. Rather, the dysphoria is a signal that an underlying issue needs addressing, and resilience and/or self-acceptance needs to be built.”
- Ayad 4/2021 podcast episode, Gender Dysphoria in Boys: Part I
- “Many presume that ROGD only impacts girls, but there is a significant number of boys who appear to show the hallmark traits of Rapid-Onset Gender Dysphoria. Not quite fitting in with Ray Blanchard’s classification of homosexual transsexualism or autogynephilia, these boys tend to be softly spoken Mommy’s boys, highly intelligent and hyper-ruminative. Many prefer to remain safe at home in their bedrooms and become fixated on medical transition. In this first of two episodes, Stella and Sasha introduce some of the different ways that gender dysphoria can manifest in boys.”
- Marchiano 2015 Layers of meaning: A Jungian analyst questions the identity model for trans-identified youth
- “A late transitioning MtT autogynephile has an experience of gender dysphoria that is vastly different than that of a fifteen-year old lesbian, and the former’s experience ought not in any way to dictate how we understand or treat the latter.”
Other Questionable Claims
- McHugh
- Blanchard
- Gynandromorphopilia: created diagnosis-“men with sexual interest in transvestites, transsexuals, and she-males”
Claim: “We’re being ‘silenced.'”
- Blanchard/Bailey: 2017 Gender dysphoria is not one thing blog post on 4thWaveNow
- “Yet a numbe rof vocal transgenderactivists who have histories typical of autogynephilic gender dysphorics do not hesitate to pressure parents, legislators, and clinicians for acquiescence, laws, and therapies that do not distinguish among types of gender dysphoric children. Moreover, they not infrequently claim inside knowledge based on their own experiences. Yet their experiences are irrelevant to the two types of gender dysphoria that they don’t have. And even with respect to autogynephilia, these transgender activists are nearly all in denial.”
- Ayad: 2018 Towards a more nuanced exploration: An interview with Sasha Ayad (4th Wave Now)
- “In recent times whenever skeptical, intelligent, and nuanced articles about transgender children appear, there’s often a dangerously aggressive and thoughtless effort to dismiss and diminish important arguments. The way things are going, I would not be surprised if things “get worse before they get better.” That being said, I am not worried about the work I’m doing because I believe it to be the right thing to do. Standing up for ethics is easy until it’s not. I am deeply committed to standing up for individualized treatment, nuanced assessment, and a least-invasive-first approach, even if that means it puts me at some personal/professional risk.”
Claim: It’s Mental Illness, You’re Not Trans
- Blanchard/Bailey: 2017 Gender dysphoria is not one thing blog post on 4thWaveNow
- “We believe that ROGD is a socially contagious phenomenon in which a young person–typically a natal female–comes to believe that she has a condition that she does not have. ROGD is not about discovering gender dysphoria that was there all along; rather, it is about falsely coming to believe that one’s problems have been due to gender dysphoria previously hidden (from the self and others).”
- Ayad: 2019 The Same but Different: Convergent Pathways of Gender Dysphoria
- “Even gender-affirmative clinicians have suspected that the male-identity in dysphoric females operates as a dissociative coping mechanism.”
- Marchiano 2018 Transgenderism and the Social Construction of Diagnosis
- “As a therapist, I have spoken with hundreds of parents of teens who have announced a trans identity “out of the blue,” and I can corroborate Littman’s initial findings. The majority of these parents have a daughter aged 14 or 15 – an age at which teens are particularly susceptible to peer influence. These teens often have one or more of the following factors that contribute to their social struggles: they are academically gifted; they are on the autism spectrum; they are same-sex attracted; they have experienced trauma or major disruption; they have other mental health diagnoses such as anxiety or depression; they have a learning disability.”
- McHugh 2019 Psychiatrist Compares Experiments on Children Claiming to Be Transgender to ‘Frontal Lobotomies’
- “McHugh said he believes, for many of these young people, mental illness precedes their gender identity disturbances.”I think their mental problems, often depression, discouragement, are the things that need treatment,” he explained, adding: I’m not positive about this. It’s a hypothesis, but it is a very plausible hypothesis, and it would explain why many of the people who go on to have treatment of their body discover they are just as depressed, discouraged and live just as problematic lives as they did before because they did not address the primary problem.”
- Malone 2019 No One Is Born in the Wrong Body
- “It should be noted that these scenarios don’t apply to all cases of gender dysphoria, as many other triggers are described in the literature. But in most cases, counseling can help gender dysphoric adolescents resolve any trauma or thought processes that have caused them to desire an opposite sexed body.”
- Laidlaw 2018 Gender Dysphoria and Children: An Endocrinologist’s Evaluation of I am Jazz
- “Sadly, many people who identify as transgender never find out until it is too late that their gender dysphoria is actually closely tied in with a mental health condition.”
.
- “Sadly, many people who identify as transgender never find out until it is too late that their gender dysphoria is actually closely tied in with a mental health condition.”
Claim: Being Trans is Like (Insert Mental Health Disorder)
- Blanchard/Bailey: 2017 Gender dysphoria is not one thing blog post on 4thWaveNow
- Recalled Memory Syndrome (RM/MPD): “Here are the main similarities between ROGD and RM/MPD: rare before 1980s; became an epidemic; primarily affecting young females; also similar to Salem witch trials; “true believers” are contradicted by past experience, common sense, and science. In ROGD, the infection route appears to be primarily directly from youngster to youngster”
- McHugh 2011 Controversial Therapy for Pre-Teen Transgender Patient Raises Questions. Fox News
- “This is child abuse. It’s like performing liposuction on an anorexic child… It is a disorder of the mind. Not a disorder of the body. Dealing with it in this way is not dealing with the problem that truly exists.”
- Lappert 2021 Doctor: Time for transgender treatment industry to “follow the science”
- “If a parent brought their son to Dr. Ladinsky and said, he is suicidal because he “has always known on the inside that he is supposed to be an offensive lineman for Alabama, but at age 16 he is skinny and weak, the law prevents Dr. Ladinsky from prescribing anabolic steroids and testosterone. This is no different.”
Misinterpretations/Mischaracterizations
- Laidlaw: 2019, Gender Dysphoria Resource for Providers
- Gender Identity = Gender Non-Conformity: “There are individuals who suffer from gender dysphoria (GD), which is an uncomfortableness about being biologically male or being biologically female, in relationship to societal expectations of gender roles. Another way to say this is that GD is a feeling of distress at being gender non-conforming. A masculine adolescent girl with preferences for more stereotypical male activities, dress, and mannerisms, for example, may become distressed at the disconnect between her gender expression and her female appearing physical body. GD can be mild to severe, and its onset can occur at any time, but classically before puberty, or peri-puberty.”
- Ayad 2021 A Counselor Explains How Conversion Therapy Bans Can Cause Harm
- Affirmative Therapy = Ignore All Other Concerns: “Affirmative therapy for gender identity refuses to consider if past trauma, eating disorders, family conflicts, autism spectrum disorder, depression, or anxiety may be contributing to a young person’s gender struggles. It’s a true disservice to the integrity of psychological therapy if clinicians blindly support cross-sex hormones, breast removal, hysterectomy or SRS for severely distressed patients.”
- Marchiano: 2017 “Outbreak: On Transgender Teens and Psychic Epidemics” (Psychological Perspectives)
- Gender Ideology = Binary Sex Stereotypes: “There is evidence that some parents may feel more comfortable having a “straight” transgender child rather than a gay or lesbian child, and are therefore supporting their child to transition.”
- Trans People are Heterosexual: “The ideology surrounding debates about transgenderism tends to be regressive, often invoking rigid sex role stereotypes. When trans-identified individuals are asked how they know they are transgender, they often answer by referencing sex role stereotypes.”
“Experts”?
- Hruz: 2017 Amicus brief filed with US District Court in Jacksonville, Florida-transgender high school student denied access to boys’ restroom
- “Dr. Hruz is an endocrinologist with purportedly “extensive experience in treating infants and children with disorders of sexual development.” Dr. Hruz, however, admits to having zero experience treating transgender patients for gender dysphoria.”
- Laidlaw: no education or experience dealing with trans children
- Ayad: 2018 Towards a more nuanced exploration: An interview with Sasha Ayad (4th Wave Now)
- “My interest in this population developed and grew organically out of my own desire to better understand the growing phenomenon. When I was a young graduate student, my understanding of this issue was limited and I was marginally familiar with the conventional, textbook examples of childhood gender dysphoria: a person, who from a very young age, is completely convinced their body is the “wrong sex.” In these cases, the wrong body self-concept develops, seemingly independent of societal norms and environmental influences. I used to think, “what a strange and troubling experience: to really believe you have the wrong sexed body.”
- McHugh 2017 Human Rights Campaign Response to Amicus Brief of Paul R. McHugh, M.D., et al. in Support of Defendant-Appellee
- “Simply being a medical doctor or researcher does not make someone an authority on transgender children. In the United States alone, dozens of experts have dedicated their careers to the health of transgender children and adolescents, drawing on clinical experience and a growing body of evidence to guide children and families. In contrast, Paul McHugh and his coauthors boast a total of zero peer-reviewed research articles on transgender people of any age. It is not clear that they have so much as met a transgender child.”
- Marchiano is a writer and therapist in private practice. She has been in contact with hundreds of parents of trans-identifying young people.
Claim: “Being Trans Is a Mental Illness
- Blanchard: 2019 Twitter thread: “Transsexualism and milder forms of gender dysphoria are types of mental disorder.”
- Malone: 2019 No Child is Born in the Wrong Body … and other thoughts on the concept of gender identity
- “Counseling can help gender dysphoric adolescents resolve any trauma or thought processes that have caused them to desire an opposite sexed body.”
- Lappert: 2018 Transgender Surgery & Catholic Anthropology
- “Transgender: Obsessive thinking with varying degrees of “dysphoria”; Perceiving something that is not objectively there: delusional thinking, errors of assumption”
- Ayad 2021. Psychotherapy May Help Trans-Curious Teens Feel More Comfortable With Their Decision
- “Through therapy, teens can explore and find a deeper understanding of themselves, process any potential trauma that may be causing this desire to transition, and how their own view of themselves matches or doesn’t match others. Therapy can also help teens learn how to have difficult conversations with others about who they are and how they identify.”
- Laidlaw 2018 The Gender Identity Phantom
- “There is apparently something called a “gender identity” which is “a person’s deep internal sense of being female, male, a combination of both, somewhere in between or neither”. This is a fantasy or superstitious belief.”
- McHugh 2020 Johns Hopkins Psychiatrist: Transgender is ‘Mental Disorder;’ Sex Change ‘Biologically Impossible’
- “policy makers and the media are doing no favors either to the public or the transgendered by treating their confusions as a right in need of defending rather than as a mental disorder that deserves understanding, treatment and prevention.”
Addendum: Clarifications and corrections
One sentence in this post was not sufficiently clear and has led to criticism. Dr. Eckert wrote:
In 2004, [Bailey was] found to be practicing without a license as a clinical psychologist.
In order to be more precise, this was changed to:
In 2004 Bailey was accused of providing clinical psychology services without a license in the form of letters of support for patients for sex reassignment surgery (SRS). These claims were apparently not pursued by the State of Illinois because Bailey did not charge for these services and therefore his actions were not illegal in the State of Illinois.)
Alice Dreger describes the incident thusly:
The charges of misconduct against Bailey are worth considering at length, and so I do that in the next part of this article, remaining here focused on the history of the backlash itself. But I will note here what I can of the outcomes of the formal complaints. It appears that the Illinois Department of Professional Regulation did not do anything with the complaint that Bailey was practicing clinical psychology without a license, presumably because he never took money for the SRS letters he wrote, nor did he offer or represent a therapeutic relationship (Clinical Psychologist Licensing Act, 225 ILCS 15/1 et. Seq.).
And:
Thus, during the time in question here, respected surgeons performing SRS typically required patients to produce evidence from two qualified psychological professionals that the applicant fit HBIGDA’s eligibility and readiness criteria for SRS.
Sometime around 1996, Kieltyka asked Bailey whether he would help out some of her friends and protégés by providing them with letters in support of their requests for SRS. Bailey was amenable to Kieltyka’s request. His understanding was that, so long as he made clear in his letters what his professional status was, there would be no problem reporting simply what he observed in terms of a pre-op transsexual woman’s gender identity presentation, her apparent understanding of the surgery, and her likelihood of adjusting well after SRS. Nowhere in his letters did Bailey say that he was these women’s therapist or that he counted under the HBIGDA Standards of Care as a “qualified mental health professional”; in each, he simply stated his university position, said how many times he had talked with the subject, and included his c.v. (Bailey, 2006b; for examples, see Conway, 2004d). Whether or not a surgeon accepted his letter as an adequate recommendation would be up to the surgeon, just as it was up to the surgeon more generally which parts of the HBIGDA Standards of Care he or she would follow.
Nowhere did Dr. Eckert claim that Bailey practiced illegally without a license, as it has been claimed in the comments that he had. However, the original phrasing was insufficiently precise.
Irreversible Damage to the Trans Community: A Critical Review of Abigail Shrier’s Irreversible Damage: The Transgender Craze Seducing Our Daughters (Part Two)
Part 2 of the review of Abigail Shrier’s “Irreversible Damage” provides insight into her harmful beliefs about trans youth, along with evidence-based counterarguments.